
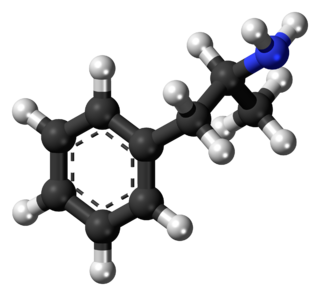
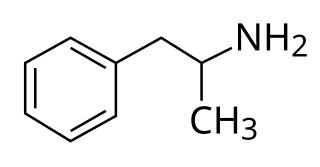
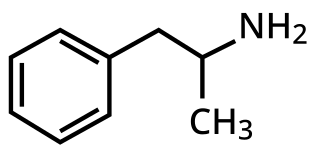
Amphetamine is a central nervous system (CNS) stimulant that is used in the treatment of attention deficit hyperactivity disorder (ADHD), narcolepsy, and obesity; it is also used to treat binge eating disorder in the form of its inactive prodrug lisdexamfetamine. Amphetamine was discovered as a chemical in 1887 by Lazăr Edeleanu, and then as a drug in the late 1920s. It exists as two enantiomers: levoamphetamine and dextroamphetamine. Amphetamine properly refers to a specific chemical, the racemic free base, which is equal parts of the two enantiomers in their pure amine forms. The term is frequently used informally to refer to any combination of the enantiomers, or to either of them alone. Historically, it has been used to treat nasal congestion and depression. Amphetamine is also used as an athletic performance enhancer and cognitive enhancer, and recreationally as an aphrodisiac and euphoriant. It is a prescription drug in many countries, and unauthorized possession and distribution of amphetamine are often tightly controlled due to the significant health risks associated with recreational use.

Stimulants are a class of drugs that increase alertness. They are used for various purposes, such as enhancing attention, motivation, cognition, mood, and physical performance. Some stimulants are naturally-occuring while others only occur synthetic. Some of the most common stimulants are caffeine, nicotine, amphetamines, cocaine, methylphenidate, and modafinil. Stimulants may be subject to varying forms of regulation, or outright prohibition, depending on jurisdiction.
The mesolimbic pathway, sometimes referred to as the reward pathway, is a dopaminergic pathway in the brain. The pathway connects the ventral tegmental area in the midbrain to the ventral striatum of the basal ganglia in the forebrain. The ventral striatum includes the nucleus accumbens and the olfactory tubercle.
Dextroamphetamine is a potent central nervous system (CNS) stimulant and enantiomer of amphetamine that is primarily prescribed for the treatment of attention deficit hyperactivity disorder (ADHD) and narcolepsy. It is also used as an athletic performance and cognitive enhancer, and recreationally as an aphrodisiac and euphoriant. Dextroamphetamine is generally regarded as the prototypical stimulant.

The nucleus accumbens is a region in the basal forebrain rostral to the preoptic area of the hypothalamus. The nucleus accumbens and the olfactory tubercle collectively form the ventral striatum. The ventral striatum and dorsal striatum collectively form the striatum, which is the main component of the basal ganglia. The dopaminergic neurons of the mesolimbic pathway project onto the GABAergic medium spiny neurons of the nucleus accumbens and olfactory tubercle. Each cerebral hemisphere has its own nucleus accumbens, which can be divided into two structures: the nucleus accumbens core and the nucleus accumbens shell. These substructures have different morphology and functions.
Adderall and Mydayis are trade names for a combination drug containing four salts of amphetamine. The mixture is composed of equal parts racemic amphetamine and dextroamphetamine, which produces a (3:1) ratio between dextroamphetamine and levoamphetamine, the two enantiomers of amphetamine. Both enantiomers are stimulants, but differ enough to give Adderall an effects profile distinct from those of racemic amphetamine or dextroamphetamine, which are marketed as Evekeo and Dexedrine/Zenzedi, respectively. Adderall is used in the treatment of attention deficit hyperactivity disorder (ADHD) and narcolepsy. It is also used illicitly as an athletic performance enhancer, cognitive enhancer, appetite suppressant, and recreationally as a euphoriant. It is a central nervous system (CNS) stimulant of the phenethylamine class.

Levmetamfetamine, also known as l-desoxyephedrine or levomethamphetamine, and commonly sold under the brand name Vicks VapoInhaler among others, is an optical isomer of methamphetamine primarily used as a topical nasal decongestant. It is used to treat nasal congestion from allergies and the common cold. It was first used medically as decongestant beginning in 1958 and has been used for such purposes, primarily in the United States, since then.
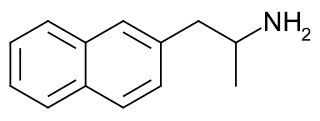
Naphthylaminopropane, also known as naphthylisopropylamine (NIPA), is an experimental drug that was under investigation for the treatment of alcohol and stimulant addiction.

Trace amine-associated receptor 1 (TAAR1) is a trace amine-associated receptor (TAAR) protein that in humans is encoded by the TAAR1 gene. TAAR1 is an intracellular amine-activated Gs-coupled and Gq-coupled G protein-coupled receptor (GPCR) that is primarily expressed in several peripheral organs and cells, astrocytes, and in the intracellular milieu within the presynaptic plasma membrane of monoamine neurons in the central nervous system (CNS). TAAR1 was discovered in 2001 by two independent groups of investigators, Borowski et al. and Bunzow et al. TAAR1 is one of six functional human trace amine-associated receptors, which are so named for their ability to bind endogenous amines that occur in tissues at trace concentrations. TAAR1 plays a significant role in regulating neurotransmission in dopamine, norepinephrine, and serotonin neurons in the CNS; it also affects immune system and neuroimmune system function through different mechanisms.

Protein fosB, also known as FosB and G0/G1 switch regulatory protein 3 (G0S3), is a protein that in humans is encoded by the FBJ murine osteosarcoma viral oncogene homolog B (FOSB) gene.
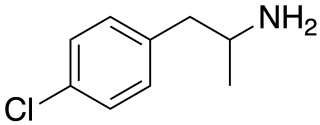
para-Chloroamphetamine (PCA), also known as 4-chloroamphetamine (4-CA), is a serotonin–norepinephrine–dopamine releasing agent (SNDRA) and serotonergic neurotoxin of the amphetamine family. It is used in scientific research in the study of the serotonin system, as a serotonin releasing agent (SRA) at lower doses to produce serotonergic effects, and as a serotonergic neurotoxin at higher doses to produce long-lasting depletions of serotonin.

MDAI, also known as 5,6-methylenedioxy-2-aminoindane, is an entactogen drug of the 2-aminoindane group which is related to MDMA and produces similar subjective effects.
A monoamine releasing agent (MRA), or simply monoamine releaser, is a drug that induces the release of one or more monoamine neurotransmitters from the presynaptic neuron into the synapse, leading to an increase in the extracellular concentrations of the neurotransmitters and hence enhanced signaling by those neurotransmitters. The monoamine neurotransmitters include serotonin, norepinephrine, and dopamine; MRAs can induce the release of one or more of these neurotransmitters.
A dopamine releasing agent (DRA) is a type of drug which induces the release of dopamine in the body and/or brain.

Amphetamine dependence refers to a state of psychological dependence on a drug in the amphetamine class. Stimulants such as amphetamines and cocaine do not cause somatic symptoms upon cessation of use but rather neurological-based mental symptoms.

Addiction is a neuropsychological disorder characterized by a persistent and intense urge to use a drug or engage in a behavior that produces natural reward, despite substantial harm and other negative consequences. Repetitive drug use often alters brain function in ways that perpetuate craving and weakens self-control. This phenomenon – drugs reshaping brain function – has led to an understanding of addiction as a brain disorder with a complex variety of psychosocial as well as neurobiological factors that are implicated in the development of addiction.
Treatment and management of addiction encompass the range of approaches aimed at helping individuals overcome addiction, most commonly in the form of substance use disorders and behavioral addictions. Effective treatment often includes a combination of medical, psychological, and social interventions tailored to the specific needs of the individual. Common practices to this end include detoxification, counseling, behavioral therapy, medication-assisted treatment, and support groups. The goal of addiction treatment is to reduce dependence, improve quality of life, and ultimately support long-term recovery. Comprehensive management addresses both the physical and psychological aspects of addiction, recognizing it as a chronic but treatable condition.
Amphetamine type stimulants (ATS) are a group of synthetic drugs that are chemical derivatives of the parent compound alpha-methylphenethylamine, also known as amphetamine. Common ATS includes amphetamine, methamphetamine, ephedrine, pseudoephedrine, 3,4-methylenedioxymethamphetamine (MDMA), 3,4-methylenedioxyamphetamine (MDA) and 3,4-methylenedioxyethylamphetamine (MDEA). ATS when used illicitly has street names including ice, meth, crystal, crank, bennies, and speed. Within the group of amphetamine-type stimulants, there are also prescription drugs including mixed amphetamine salts, dextroamphetamine, and lisdexamfetamine.
Disorders of diminished motivation (DDM) are a group of disorders involving diminished motivation and associated emotions. Many different terms have been used to refer to diminished motivation. Often however, a spectrum is defined encompassing apathy, abulia, and akinetic mutism, with apathy the least severe and akinetic mutism the most extreme.
RO5203648 is a trace amine-associated receptor 1 (TAAR1) partial agonist. It is a potent and highly selective partial agonist of both rodent and primate TAAR1. The drug suppresses the effects of psychostimulants like cocaine and methamphetamine. It also produces a variety of other behavioral effects, such as antidepressant-like, antipsychotic-like, and antiaddictive effects. Research with RO5203648 has led to interest in TAAR1 agonists for potential treatment of drug addiction. RO5203648 itself was not developed for potential medical use due to poor expected human pharmacokinetics.

















