
Mouthwash, mouth rinse, oral rinse, or mouth bath is a liquid which is held in the mouth passively or swirled around the mouth by contraction of the perioral muscles and/or movement of the head, and may be gargled, where the head is tilted back and the liquid bubbled at the back of the mouth.

Human teeth function to mechanically break down items of food by cutting and crushing them in preparation for swallowing and digesting. As such, they are considered part of the human digestive system. Humans have four types of teeth: incisors, canines, premolars, and molars, which each have a specific function. The incisors cut the food, the canines tear the food and the molars and premolars crush the food. The roots of teeth are embedded in the maxilla or the mandible and are covered by gums. Teeth are made of multiple tissues of varying density and hardness.
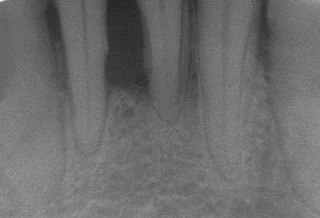
Periodontal disease, also known as gum disease, is a set of inflammatory conditions affecting the tissues surrounding the teeth. In its early stage, called gingivitis, the gums become swollen and red and may bleed. It is considered the main cause of tooth loss for adults worldwide. In its more serious form, called periodontitis, the gums can pull away from the tooth, bone can be lost, and the teeth may loosen or fall out. Halitosis may also occur.

A toothbrush is a special type of brush used to clean the teeth, gums, and tongue. It consists of a head of tightly clustered bristles, atop of which toothpaste can be applied, mounted on a handle which facilitates the cleaning of hard-to-reach areas of the mouth. They should be used in conjunction with something to clean between the teeth where the bristles of the toothbrush cannot reach - for example floss, tape or interdental brushes.

Toothpaste is a paste or gel dentifrice used with a toothbrush to clean and maintain the aesthetics and health of teeth. Toothpaste is used to promote oral hygiene: it is an abrasive that aids in removing dental plaque and food from the teeth, assists in suppressing halitosis, and delivers active ingredients to help prevent tooth decay and gum disease (gingivitis). Owing to differences in composition and fluoride content, not all toothpastes are equally effective in maintaining oral health. The decline of tooth decay during the 20th century has been attributed to the introduction and regular use of fluoride-containing toothpastes worldwide. Large amounts of swallowed toothpaste can be poisonous. Common colors for toothpaste include white and blue.
Teeth cleaning is part of oral hygiene and involves the removal of dental plaque from teeth with the intention of preventing cavities, gingivitis, and periodontal disease. People routinely clean their own teeth by brushing and interdental cleaning, and dental hygienists can remove hardened deposits (tartar) not removed by routine cleaning. Those with dentures and natural teeth may supplement their cleaning with a denture cleaner.

Tooth decay, also known as cavities or caries, is the breakdown of teeth due to acids produced by bacteria. The cavities may be a number of different colors, from yellow to black. Symptoms may include pain and difficulty eating. Complications may include inflammation of the tissue around the tooth, tooth loss and infection or abscess formation. Tooth regeneration is an ongoing stem cell–based field of study that aims to find methods to reverse the effects of decay; current methods are based on easing symptoms.
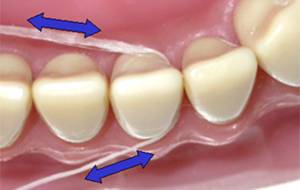
Dental floss is a cord of thin filaments, typically made of nylon or silk, used in interdental cleaning to remove food and dental plaque from between teeth or places a toothbrush has difficulty reaching or is unable to reach. Its regular use as part of oral cleaning is intended to maintain oral health.
Periodontology or periodontics is the specialty of dentistry that studies supporting structures of teeth, as well as diseases and conditions that affect them. The supporting tissues are known as the periodontium, which includes the gingiva (gums), alveolar bone, cementum, and the periodontal ligament. A periodontist is a dentist that specializes in the prevention, diagnosis and treatment of periodontal disease and in the placement of dental implants.
Dental plaque is a biofilm of microorganisms that grows on surfaces within the mouth. It is a sticky colorless deposit at first, but when it forms tartar, it is often brown or pale yellow. It is commonly found between the teeth, on the front of teeth, behind teeth, on chewing surfaces, along the gumline (supragingival), or below the gumline cervical margins (subgingival). Dental plaque is also known as microbial plaque, oral biofilm, dental biofilm, dental plaque biofilm or bacterial plaque biofilm. Bacterial plaque is one of the major causes for dental decay and gum disease.

An oral irrigator is a home dental care device which uses a stream of high-pressure pulsating water intended to remove dental plaque and food debris between teeth and below the gum line. Regular use of an oral irrigator is believed to improve gingival health. The devices may also provide easier cleaning for braces and dental implants. However, more research is needed to confirm plaque biofilm removal and effectiveness when used by patients with special oral or systemic health needs.

Tooth brushing is the act of scrubbing teeth with a toothbrush equipped with toothpaste. Interdental cleaning can be useful with tooth brushing, and together these two activities are the primary means of cleaning teeth, one of the main aspects of oral hygiene. The recommended amount of time for tooth brushing is two minutes.
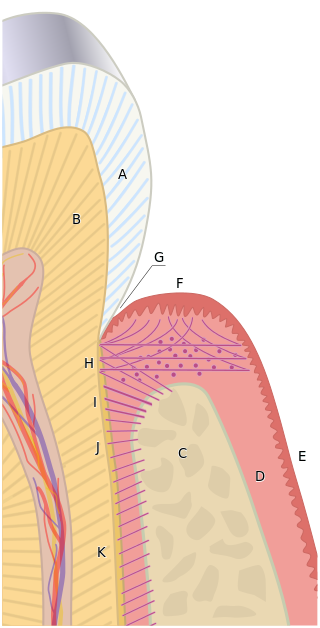
In dental anatomy, the gingival and periodontal pockets are dental terms indicating the presence of an abnormal depth of the gingival sulcus near the point at which the gingival (gum) tissue contacts the tooth.

Scaling and root planing, also known as conventional periodontal therapy, non-surgical periodontal therapy or deep cleaning, is a procedure involving removal of dental plaque and calculus and then smoothing, or planing, of the (exposed) surfaces of the roots, removing cementum or dentine that is impregnated with calculus, toxins, or microorganisms, the agents that cause inflammation. It is a part of non-surgical periodontal therapy. This helps to establish a periodontium that is in remission of periodontal disease. Periodontal scalers and periodontal curettes are some of the tools involved.
Dental Public Health (DPH) is a para-clinical specialty of dentistry that deals with the prevention of oral disease and promotion of oral health. Dental public health is involved in the assessment of key dental health needs and coming up with effective solutions to improve the dental health of populations rather than individuals.

A tongue cleaner is an oral hygiene device designed to clean the coating on the upper surface of the tongue. While there is tentative benefit from the use of a tongue cleaner it is insufficient to draw clear conclusions regarding bad breath.

Gingivitis is a non-destructive disease that causes inflammation of the gums; ulitis is an alternative term. The most common form of gingivitis, and the most common form of periodontal disease overall, is in response to bacterial biofilms that are attached to tooth surfaces, termed plaque-induced gingivitis. Most forms of gingivitis are plaque-induced.
Gingival disease is a term used to group the diseases that affect the gingiva(gums). The most common gingival disease is gingivitis, the earliest stage of gingival-related diseases. Gingival disease encompasses all the conditions that surround the gums, this includes plaque-induced gingivitis, non-dental biofilm plaque-induced gingivitis, and periodontal diseases.

Tooth pathology is any condition of the teeth that can be congenital or acquired. Sometimes a congenital tooth disease is called a tooth abnormality. These are among the most common diseases in humans The prevention, diagnosis, treatment and rehabilitation of these diseases are the base to the dentistry profession, in which are dentists and dental hygienists, and its sub-specialties, such as oral medicine, oral and maxillofacial surgery, and endodontics. Tooth pathology is usually separated from other types of dental issues, including enamel hypoplasia and tooth wear.
Interdental cleaning or interproximal cleaning is part of oral hygiene where the aim is to clean the areas in between the teeth, otherwise known as the proximal surfaces of teeth. This is to remove the dental plaque in areas a toothbrush cannot reach. The ultimate goal of interproximal cleaning is to prevent the development of interproximal caries and periodontal disease. The combined use of tooth brushing, and mechanical and manual interdental cleaning devices has been proven to reduce the prevalence of caries and periodontal diseases.




