
Methadone, sold under the brand names Dolophine and Methadose among others, is a synthetic opioid used medically to treat chronic pain and opioid use disorder. Prescribed for daily use, the medicine relieves cravings and opioid withdrawal symptoms. Withdrawal management using methadone can be accomplished in less than a month, or it may be done gradually over a longer period of time, or simply maintained for the rest of the patient's life. While a single dose has a rapid effect, maximum effect can take up to five days of use. After long-term use, in people with normal liver function, effects last 8 to 36 hours. Methadone is usually taken by mouth and rarely by injection into a muscle or vein.
Oxycodone, sold under the brand name Roxicodone and OxyContin among others, is a semi-synthetic opioid used medically for the treatment of moderate to severe pain. It is highly addictive and is a commonly abused drug. It is usually taken by mouth, and is available in immediate-release and controlled-release formulations. Onset of pain relief typically begins within fifteen minutes and lasts for up to six hours with the immediate-release formulation. In the United Kingdom, it is available by injection. Combination products are also available with paracetamol (acetaminophen), ibuprofen, naloxone, naltrexone, and aspirin.

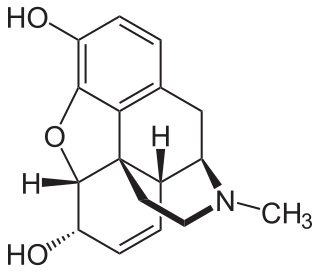
Hydromorphone, also known as dihydromorphinone, and sold under the brand name Dilaudid among others, is a morphinan opioid used to treat moderate to severe pain. Typically, long-term use is only recommended for pain due to cancer. It may be used by mouth or by injection into a vein, muscle, or under the skin. Effects generally begin within half an hour and last for up to five hours. A 2016 Cochrane review found little difference in benefit between hydromorphone and other opioids for cancer pain.
Opioids are a class of drugs that derive from, or mimic, natural substances found in the opium poppy plant. Opioids work in the brain to produce a variety of effects, including pain relief. As a class of substances, they act on opioid receptors to produce morphine-like effects.
Opioid use disorder (OUD) is a substance use disorder characterized by cravings for opioids, continued use despite physical and/or psychological deterioration, increased tolerance with use, and withdrawal symptoms after discontinuing opioids. Opioid withdrawal symptoms include nausea, muscle aches, diarrhea, trouble sleeping, agitation, and a low mood. Addiction and dependence are important components of opioid use disorder.

Buprenorphine, sold under the brand name Subutex among others, is an opioid used to treat opioid use disorder, acute pain, and chronic pain. It can be used under the tongue (sublingual), in the cheek (buccal), by injection, as a skin patch (transdermal), or as an implant. For opioid use disorder, the patient must have moderate opioid withdrawal symptoms before buprenorphine can be administered under direct observation of a health-care provider.
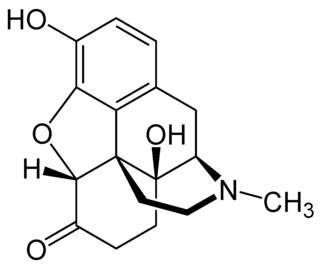
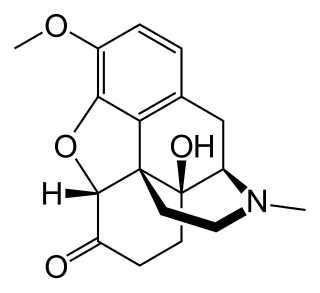
Oxymorphone is a highly potent opioid analgesic indicated for treatment of severe pain. Pain relief after injection begins after about 5–10 minutes, after oral administration it begins after about 30 minutes, and lasts about 3–4 hours for immediate-release tablets and 12 hours for extended-release tablets. The elimination half-life of oxymorphone is much faster intravenously, and as such, the drug is most commonly used orally. Like oxycodone, which metabolizes to oxymorphone, oxymorphone has a high potential to be abused.
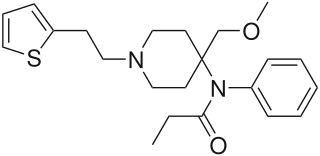
Sufentanil, sold under the brand names Sufenta among others, is a synthetic opioid analgesic drug approximately 5 to 10 times as potent as its parent drug, fentanyl, and 500 to 1,000 times as potent as morphine. Structurally, sufentanil differs from fentanyl through the addition of a methoxymethyl group on the piperidine ring, and the replacement of the phenyl ring by thiophene. Sufentanil first was synthesized at Janssen Pharmaceutica in 1974.

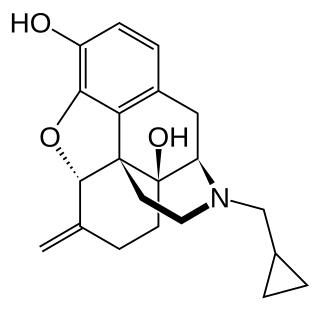
Naltrexone, sold under the brand name Revia among others, is a medication primarily used to manage alcohol use or opioid use disorder by reducing cravings and feelings of euphoria associated with substance use disorder. It has also been found effective in the treatment of other addictions and may be used for them off-label. An opioid-dependent person should not receive naltrexone before detoxification. It is taken orally or by injection into a muscle. Effects begin within 30 minutes, though a decreased desire for opioids may take a few weeks to occur.
Nalmefene, sold under the brand name Revex among others, is a medication that is used in the treatment of opioid overdose and alcohol dependence. Nalmefene belongs to the class of opioid antagonists and can be taken by mouth, administered by injection, or delivered through nasal administration.
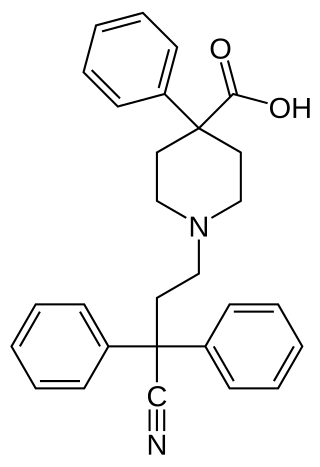
Difenoxin is an opioid drug used, often in combination with atropine, to treat diarrhea. It is the principal metabolite of diphenoxylate.
An equianalgesic chart is a conversion chart that lists equivalent doses of analgesics. Equianalgesic charts are used for calculation of an equivalent dose between different analgesics. Tables of this general type are also available for NSAIDs, benzodiazepines, depressants, stimulants, anticholinergics and others.

An opioid overdose is toxicity due to excessive consumption of opioids, such as morphine, codeine, heroin, fentanyl, tramadol, and methadone. This preventable pathology can be fatal if it leads to respiratory depression, a lethal condition that can cause hypoxia from slow and shallow breathing. Other symptoms include small pupils and unconsciousness; however, its onset can depend on the method of ingestion, the dosage and individual risk factors. Although there were over 110,000 deaths in 2017 due to opioids, individuals who survived also faced adverse complications, including permanent brain damage.
Buprenorphine/naloxone, sold under the brand name Suboxone among others, is a fixed-dose combination medication that includes buprenorphine and naloxone. It is used to treat opioid use disorder, and reduces the mortality of opioid use disorder by 50%. It relieves cravings to use and withdrawal symptoms. Buprenorphine/naloxone is available for use in two different forms, under the tongue or in the cheek.
The California State Legislature passed an act to amend Section 1714.22 of the Civil Code, relating to drug overdose treatment in 2014. California Assembly Bill 1535 (2014) delegated the authority to all properly licensed California state pharmacists who had undergone a training program of at least one hour of continuing education about the pharmacology of naloxone hydrochloride to dispense naloxone under standards developed by the Medical Board of California in conjunction with the California Society of Addiction Medicine, the California Pharmacists Association, and any other appropriate entities.

There is an ongoing opioid epidemic in the United States, originating out of both medical prescriptions and illegal sources. It has been called "one of the most devastating public health catastrophes of our time". The opioid epidemic unfolded in three waves. The first wave of the epidemic in the United States began in the late 1990s, according to the Centers for Disease Control and Prevention (CDC), when opioids were increasingly prescribed for pain management, resulting in a rise in overall opioid use throughout subsequent years. The second wave was from an expansion in the heroin market to supply already addicted people. The third wave, starting in 2013, was marked by a steep tenfold increase in the synthetic opioid-involved death rate as synthetic opioids flooded the US market.
Phil Skolnick is an American neuroscientist and pharmacologist most widely known for his work on the psychopharmacology of depression and anxiety, as well as on addiction medicine. Author of more than 500 published papers, Skolnick's most notable accomplishments include elucidating the role of the NMDA system in depression therapeutics, demonstrating the existence of endogenous benzodiazepine receptor ligands, and spearheading the National Institute on Drug Abuse's partnership to develop a naloxone atomizer for reversal of acute opioid overdose. Skolnick's work also laid the foundation for the development of ketamine as a rapid-acting antidepressant.
AptarGroup, Inc., also known as Aptar, is a United States–based global manufacturer of consumer dispensing packaging and drug delivery devices. The group has manufacturing operations in 18 countries.

Opioid withdrawal is a set of symptoms arising from the sudden cessation or reduction of opioids where previous usage has been heavy and prolonged. Signs and symptoms of withdrawal can include drug craving, anxiety, restless legs syndrome, nausea, vomiting, diarrhea, sweating, and an elevated heart rate. Opioid use triggers a rapid adaptation in cellular signaling pathways that, when reduced or stopped, can cause adverse physiological effects. All opioids, both recreational drugs and medications, when reduced or stopped, can lead to opioid withdrawal symptoms. When withdrawal symptoms are due to recreational opioid use, the term opioid use disorder is used, whereas when due to prescribed medications, the term prescription opioid use disorder is used. Opioid withdrawal can be managed by the use of opioid replacement therapy, while symptoms may be relieved by the use of medications such as lofexidine and clonidine.
In response to the surging opioid prescription rates by health care providers that contributed to the opioid epidemic in the United States, US states began passing legislation to stifle high-risk prescribing practices. These new laws fell primarily into one of the following four categories:
- Prescription Drug Monitoring Program (PDMP) enrollment laws: prescribers must enroll in their state's PDMP, an electronic database containing a record of all patients' controlled substance prescriptions
- PDMP query laws: prescribers must check the PDMP before prescribing an opioid
- Opioid prescribing cap laws: opioid prescriptions cannot exceed designated doses or durations
- Pill mill laws: pain clinics are closely regulated and monitored to minimize the prescription of opioids non-medically





