
In human anatomy, the wrist is variously defined as (1) the carpus or carpal bones, the complex of eight bones forming the proximal skeletal segment of the hand; (2) the wrist joint or radiocarpal joint, the joint between the radius and the carpus and; (3) the anatomical region surrounding the carpus including the distal parts of the bones of the forearm and the proximal parts of the metacarpus or five metacarpal bones and the series of joints between these bones, thus referred to as wrist joints. This region also includes the carpal tunnel, the anatomical snuff box, bracelet lines, the flexor retinaculum, and the extensor retinaculum.

The anatomical snuff box or snuffbox or foveola radialis is a triangular deepening on the radial, dorsal aspect of the hand—at the level of the carpal bones, specifically, the scaphoid and trapezium bones forming the floor. The name originates from the use of this surface for placing and then sniffing powdered tobacco, or "snuff." It is sometimes referred to by its French name tabatière.

The trapezoid bone is a carpal bone in tetrapods, including humans. It is the smallest bone in the distal row of carpal bones that give structure to the palm of the hand. It may be known by its wedge-shaped form, the broad end of the wedge constituting the dorsal, the narrow end the palmar surface; and by its having four articular facets touching each other, and separated by sharp edges. It is homologous with the "second distal carpal" of reptiles and amphibians.

The scaphoid bone is one of the carpal bones of the wrist. It is situated between the hand and forearm on the thumb side of the wrist. It forms the radial border of the carpal tunnel. The scaphoid bone is the largest bone of the proximal row of wrist bones, its long axis being from above downward, lateralward, and forward. It is approximately the size and shape of a medium cashew nut.

The capitate bone is a bone in the human wrist found in the center of the carpal bone region, located at the distal end of the radius and ulna bones. It articulates with the third metacarpal bone and forms the third carpometacarpal joint. The capitate bone is the largest of the carpal bones in the human hand. It presents, above, a rounded portion or head, which is received into the concavity formed by the scaphoid and lunate bones; a constricted portion or neck; and below this, the body. The bone is also found in many other mammals, and is homologous with the "third distal carpal" of reptiles and amphibians.

The navicular bone is a small bone found in the feet of most mammals.

A Colles' fracture is a type of fracture of the distal forearm in which the broken end of the radius is bent backwards. Symptoms may include pain, swelling, deformity, and bruising. Complications may include damage to the median nerve.
A distal radius fracture, also known as wrist fracture, is a break of the part of the radius bone which is close to the wrist. Symptoms include pain, bruising, and rapid-onset swelling. The ulna bone may also be broken.

Avascular necrosis (AVN), also called osteonecrosis or bone infarction, is death of bone tissue due to interruption of the blood supply. Early on, there may be no symptoms. Gradually joint pain may develop, which may limit the person's ability to move. Complications may include collapse of the bone or nearby joint surface.
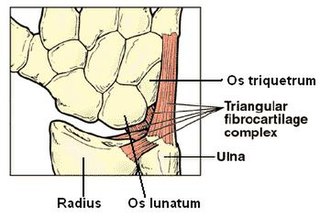
The triangular fibrocartilage complex (TFCC) is formed by the triangular fibrocartilage discus (TFC), the radioulnar ligaments (RULs) and the ulnocarpal ligaments (UCLs).

The midcarpal joint is formed by the scaphoid, lunate, and triquetral bones in the proximal row, and the trapezium, trapezoid, capitate, and hamate bones in the distal row. The distal pole of the scaphoid articulates with two trapezial bones as a gliding type of joint. The proximal end of the scaphoid combines with the lunate and triquetrum to form a deep concavity that articulates with the convexity of the combined capitate and hamate in a form of diarthrodial, almost condyloid joint.

Percutaneous pinning is a technique used by orthopedic and podiatric surgeons for the stabilization of unstable fractures. Percutaneous pinning involves inserting wires through a person's skin for stabilizing the fractured bone.
Preiser disease, or (idiopathic) avascular necrosis of the scaphoid, is a rare condition where ischemia and necrosis of the scaphoid bone occurs without previous fracture. It is thought to be caused by repetitive microtrauma or side effects of drugs in conjunction with existing defective vascular supply to the proximal pole of the scaphoid. MRI coupled with CT and X-ray are the methods of choice for diagnosis.

Bennett fracture is a type of partial broken finger involving the base of the thumb, and extends into the carpometacarpal (CMC) joint.

A humerus fracture is a break of the humerus bone in the upper arm. Symptoms may include pain, swelling, and bruising. There may be a decreased ability to move the arm and the person may present holding their elbow. Complications may include injury to an artery or nerve, and compartment syndrome.

The scapholunate ligament is a ligament of the wrist.

A hand is a prehensile, multi-fingered appendage located at the end of the forearm or forelimb of primates such as humans, chimpanzees, monkeys, and lemurs. A few other vertebrates such as the koala are often described as having "hands" instead of paws on their front limbs. The raccoon is usually described as having "hands" though opposable thumbs are lacking.

An ulna fracture is a break in the ulna bone, one of the two bones in the forearm. It is often associated with a fracture of the other forearm bone, the radius.

Wrist osteoarthritis is gradual loss of articular cartilage and hypertrophic bone changes (osteophytes). While in many joints this is part of normal aging (senescence), in the wrist osteoarthritis usually occurs over years to decades after scapholunate interosseous ligament rupture or an unhealed fracture of the scaphoid. Characteristic symptoms including pain, deformity and stiffness. Pain intensity and incapability are notably variable and do not correspond with arthritis severity on radiographs.
An occult fracture is a fracture that is not readily visible, generally in regard to projectional radiography ("X-ray"). Radiographically, occult and subtle fractures are a diagnostic challenge. They may be divided into 1) high energy trauma fracture, 2) fatigue fracture from cyclical and sustained mechanical stress, and 3) insufficiency fracture occurring in weakened bone. Independently of the cause, the initial radiographic examination can be negative either because the findings seem normal or are too subtle. Advanced imaging tools such as computed tomography, magnetic resonance imaging (MRI), and scintigraphy are highly valuable in the early detection of these fractures.








