
Bradycardia, also called bradyarrhythmia, is a resting heart rate under 60 beats per minute (BPM). While bradycardia can result from various pathologic processes, it is commonly a physiologic response to cardiovascular conditioning or due to asymptomatic type 1 atrioventricular block.
Kocher–Debré–Semelaigne syndrome (KDSS) is hypothyroidism in infancy or childhood characterised by lower extremity or generalized muscular hypertrophy, myxoedema, short stature, and cognitive impairment.

Tachycardia, also called tachyarrhythmia, is a heart rate that exceeds the normal resting rate. In general, a resting heart rate over 100 beats per minute is accepted as tachycardia in adults. Heart rates above the resting rate may be normal or abnormal.

Glycogen storage disease type V, also known as McArdle's disease, is a metabolic disorder, one of the metabolic myopathies, more specifically a muscle glycogen storage disease, caused by a deficiency of myophosphorylase. Its incidence is reported as one in 100,000, roughly the same as glycogen storage disease type I.

A glycogen storage disease is a metabolic disorder caused by a deficiency of an enzyme or transport protein affecting glycogen synthesis, glycogen breakdown, or glucose breakdown, typically in muscles and/or liver cells.

Sinus node dysfunction (SND), also known as sick sinus syndrome (SSS), is a group of abnormal heart rhythms (arrhythmias) usually caused by a malfunction of the sinus node, the heart's primary pacemaker. Tachycardia-bradycardia syndrome is a variant of sick sinus syndrome in which the arrhythmia alternates between fast and slow heart rates.

Palpitations are perceived abnormalities of the heartbeat characterized by awareness of cardiac muscle contractions in the chest, which is further characterized by the hard, fast and/or irregular beatings of the heart.
Alkalosis is the result of a process reducing hydrogen ion concentration of arterial blood plasma (alkalemia). In contrast to acidemia, alkalemia occurs when the serum pH is higher than normal. Alkalosis is usually divided into the categories of respiratory alkalosis and metabolic alkalosis or a combined respiratory/metabolic alkalosis.
Phosphoglucomutase is an enzyme that transfers a phosphate group on an α-D-glucose monomer from the 1 to the 6 position in the forward direction or the 6 to the 1 position in the reverse direction.
Muscle fatigue is when muscles that were initially generating a normal amount of force, then experience a declining ability to generate force. It can be a result of vigorous exercise, but abnormal fatigue may be caused by barriers to or interference with the different stages of muscle contraction. There are two main causes of muscle fatigue: the limitations of a nerve’s ability to generate a sustained signal ; and the reduced ability of the muscle fiber to contract.
Postural orthostatic tachycardia syndrome (POTS) is a condition characterized by an abnormally large increase in heart rate upon sitting up or standing. POTS is a disorder of the autonomic nervous system that can lead to a variety of symptoms, including lightheadedness, brain fog, blurred vision, weakness, fatigue, headaches, heart palpitations, exercise intolerance, nausea, diminished concentration, tremulousness (shaking), syncope (fainting), coldness or pain in the extremities, numbness or tingling in the extremities, chest pain, and shortness of breath. Other conditions associated with POTS include myalgic encephalomyelitis/chronic fatigue syndrome, migraine headaches, Ehlers–Danlos syndrome, asthma, autoimmune disease, vasovagal syncope, and mast cell activation syndrome. POTS symptoms may be treated with lifestyle changes such as increasing fluid, electrolyte, and salt intake, wearing compression stockings, gentle and slow postural changes, avoiding prolonged bedrest, medication, and physical therapy.

Exercise intolerance is a condition of inability or decreased ability to perform physical exercise at the normally expected level or duration for people of that age, size, sex, and muscle mass. It also includes experiences of unusually severe post-exercise pain, fatigue, nausea, vomiting or other negative effects. Exercise intolerance is not a disease or syndrome in and of itself, but can result from various disorders.

In endurance sports such as road cycling and long-distance running, hitting the wall or the bonk is a condition of sudden fatigue and loss of energy which is caused by the depletion of glycogen stores in the liver and muscles. Milder instances can be remedied by brief rest and the ingestion of food or drinks containing carbohydrates. Otherwise, it can be remedied by attaining second wind by either resting for approximately 10 minutes or by slowing down considerably and increasing speed slowly over a period of 10 minutes. Ten minutes is approximately the time that it takes for free fatty acids to sufficiently produce ATP in response to increased demand.

Inappropriate sinus tachycardia (IST) is defined as sinus tachycardia that is not caused by identifiable medical ailments, a physiological reaction, or pharmaceuticals (a diagnosis of exclusion) and is accompanied by symptoms, frequently invalidating and affecting quality of life. IST symptoms include palpitations, chest discomfort, exhaustion, shortness of breath, presyncope, and syncope.
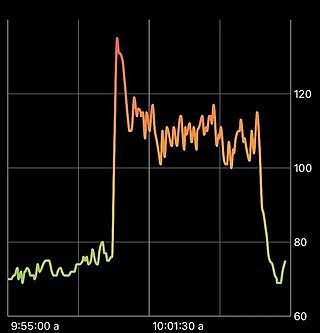
Second wind is a phenomenon in endurance sports, such as marathons or road running, whereby an athlete who is out of breath and too tired to continue, finds the strength to press on at top performance with less exertion. The feeling may be similar to that of a "runner's high", the most obvious difference being that the runner's high occurs after the race is over. In muscle glycogenoses, an inborn error of carbohydrate metabolism impairs either the formation or utilization of muscle glycogen. As such, those with muscle glycogenoses do not need to do prolonged exercise to experience "hitting the wall". Instead, signs of exercise intolerance, such as an inappropriate rapid heart rate response to exercise, are experienced from the beginning of an activity, and some muscle GSDs can achieve second wind within about 10 minutes from the beginning of the aerobic activity, such as walking. (See below in pathology).

Inborn errors of carbohydrate metabolism are inborn error of metabolism that affect the catabolism and anabolism of carbohydrates.
Syncope, commonly known as fainting or passing out, is a loss of consciousness and muscle strength characterized by a fast onset, short duration, and spontaneous recovery. It is caused by a decrease in blood flow to the brain, typically from low blood pressure. There are sometimes symptoms before the loss of consciousness such as lightheadedness, sweating, pale skin, blurred vision, nausea, vomiting, or feeling warm. Syncope may also be associated with a short episode of muscle twitching. Psychiatric causes can also be determined when a patient experiences fear, anxiety, or panic; particularly before a stressful event, usually medical in nature. When consciousness and muscle strength are not completely lost, it is called presyncope. It is recommended that presyncope be treated the same as syncope.

Metabolic myopathies are myopathies that result from defects in biochemical metabolism that primarily affect muscle. They are generally genetic defects that interfere with the ability to create energy, causing a low ATP reservoir within the muscle cell.

Arrhythmias, also known as cardiac arrhythmias, are irregularities in the heartbeat, including when it is too fast or too slow. A resting heart rate that is too fast – above 100 beats per minute in adults – is called tachycardia, and a resting heart rate that is too slow – below 60 beats per minute – is called bradycardia. Some types of arrhythmias have no symptoms. Symptoms, when present, may include palpitations or feeling a pause between heartbeats. In more serious cases, there may be lightheadedness, passing out, shortness of breath, chest pain, or decreased level of consciousness. While most cases of arrhythmia are not serious, some predispose a person to complications such as stroke or heart failure. Others may result in sudden death.
Hoffmann syndrome is a rare form of hypothyroid myopathy and is not to be confused with Werdnig-Hoffmann disease.

