
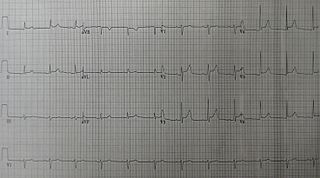
Electrocardiography is the process of producing an electrocardiogram. It is a graph of voltage versus time of the electrical activity of the heart using electrodes placed on the skin. These electrodes detect the small electrical changes that are a consequence of cardiac muscle depolarization followed by repolarization during each cardiac cycle (heartbeat). Changes in the normal ECG pattern occur in numerous cardiac abnormalities, including cardiac rhythm disturbances, inadequate coronary artery blood flow, and electrolyte disturbances.

Atrial flutter (AFL) is a common abnormal heart rhythm that starts in the atrial chambers of the heart. When it first occurs, it is usually associated with a fast heart rate and is classified as a type of supraventricular tachycardia. Atrial flutter is characterized by a sudden-onset (usually) regular abnormal heart rhythm on an electrocardiogram (ECG) in which the heart rate is fast. Symptoms may include a feeling of the heart beating too fast, too hard, or skipping beats, chest discomfort, difficulty breathing, a feeling as if one's stomach has dropped, a feeling of being light-headed, or loss of consciousness.

Second-degree atrioventricular block is a disease of the electrical conduction system of the heart. It is a conduction block between the atria and ventricles. The presence of second-degree AV block is diagnosed when one or more of the atrial impulses fail to conduct to the ventricles due to impaired conduction. It is classified as a block of the AV node and is categorized in between first-degree and third degree blocks.

Ventricular tachycardia is a type of regular, fast heart rate that arises from improper electrical activity in the ventricles of the heart. Although a few seconds may not result in problems, longer periods are dangerous. Short periods may occur without symptoms, or present with lightheadedness, palpitations, or chest pain. Ventricular tachycardia may result in ventricular fibrillation and turn into sudden death. It is found initially in about 7% of people in cardiac arrest.
A sinus rhythm is any cardiac rhythm in which depolarisation of the cardiac muscle begins at the sinus node. It is characterised by the presence of correctly oriented P waves on the electrocardiogram (ECG). Sinus rhythm is necessary, but not sufficient, for normal electrical activity within the heart.
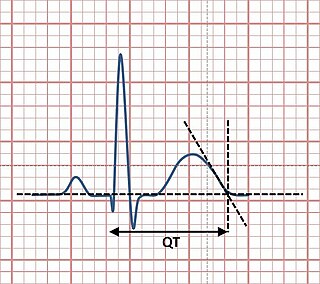
The QT interval is a measurement made on an electrocardiogram used to assess some of the electrical properties of the heart. It is calculated as the time from the start of the Q wave to the end of the T wave, and approximates to the time taken from when the cardiac ventricles start to contract to when they finish relaxing. An abnormally long or abnormally short QT interval is associated with an increased risk of developing abnormal heart rhythms and sudden cardiac death. Abnormalities in the QT interval can be caused by genetic conditions such as long QT syndrome, by certain medications such as sotalol or pitolisant, by disturbances in the concentrations of certain salts within the blood such as hypokalaemia, or by hormonal imbalances such as hypothyroidism.

Left ventricular hypertrophy (LVH) is thickening of the heart muscle of the left ventricle of the heart, that is, left-sided ventricular hypertrophy.
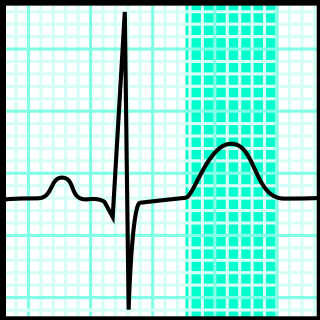
In electrocardiography, the T wave represents the repolarization of the ventricles. The interval from the beginning of the QRS complex to the apex of the T wave is referred to as the absolute refractory period. The last half of the T wave is referred to as the relative refractory period or vulnerable period. The T wave contains more information than the QT interval. The T wave can be described by its symmetry, skewness, slope of ascending and descending limbs, amplitude and subintervals like the Tpeak–Tend interval.
The QRS complex is the combination of three of the graphical deflections seen on a typical electrocardiogram. It is usually the central and most visually obvious part of the tracing; in other words, it's the main spike seen on an ECG line. It corresponds to the depolarization of the right and left ventricles of the human heart and contraction of the large ventricular muscles.

Einthoven's triangle is an imaginary formation of three limb leads in a triangle used in electrocardiography, formed by the two shoulders and the pubis. The shape forms an inverted equilateral triangle with the heart at the center. It is named after Willem Einthoven, who theorized its existence.
Acute pericarditis is a type of pericarditis usually lasting less than 6 weeks. It is the most common condition affecting the pericardium.

Electrical alternans is an electrocardiographic phenomenon of alternation of QRS complex amplitude or axis between beats and a possible wandering base-line. It is seen in cardiac tamponade and severe pericardial effusion and is thought to be related to changes in the ventricular electrical axis due to fluid in the pericardium, as the heart essentially wobbles in the fluid filled pericardial sac.
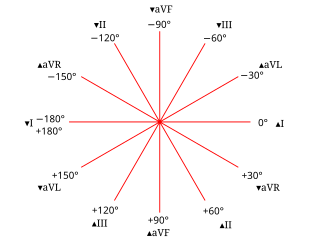
The electrical axis of the heart is the net direction in which the wave of depolarisation travels. It is measured using an electrocardiogram (ECG). Normally, this begins at the sinoatrial node ; from here the wave of depolarisation travels down to the apex of the heart. The hexaxial reference system can be used to visualise the directions in which the depolarisation wave may travel.
Left anterior fascicular block (LAFB) is an abnormal condition of the left ventricle of the heart, related to, but distinguished from, left bundle branch block (LBBB).
A left posterior fascicular block (LPFB), also known as left posterior hemiblock (LPH), is a condition where the left posterior fascicle, which travels to the inferior and posterior portion of the left ventricle, does not conduct the electrical impulses from the atrioventricular node. The wave-front instead moves more quickly through the left anterior fascicle and right bundle branch, leading to a right axis deviation seen on the ECG.

Vectorcardiography (VCG) is a method of recording the magnitude and direction of the electrical forces that are generated by the heart by means of a continuous series of vectors that form curving lines around a central point.

ST elevation refers to a finding on an electrocardiogram wherein the trace in the ST segment is abnormally high above the baseline.
In electrocardiography, left axis deviation (LAD) is a condition wherein the mean electrical axis of ventricular contraction of the heart lies in a frontal plane direction between −30° and −90°. This is reflected by a QRS complex positive in lead I and negative in leads aVF and II.

Right atrial enlargement (RAE) is a form of cardiomegaly, or heart enlargement. It can broadly be classified as either right atrial hypertrophy (RAH), overgrowth, or dilation, like an expanding balloon. Common causes include pulmonary hypertension, which can be the primary defect leading to RAE, or pulmonary hypertension secondary to tricuspid stenosis; pulmonary stenosis or Tetralogy of Fallot i.e. congenital diseases; chronic lung disease, such as Cor Pulmonale. Other recognised causes are: right ventricular failure, tricuspid regurgitation, and atrial septal defect.

Electrocardiography in suspected myocardial infarction has the main purpose of detecting ischemia or acute coronary injury in emergency department populations coming for symptoms of myocardial infarction (MI). Also, it can distinguish clinically different types of myocardial infarction.


