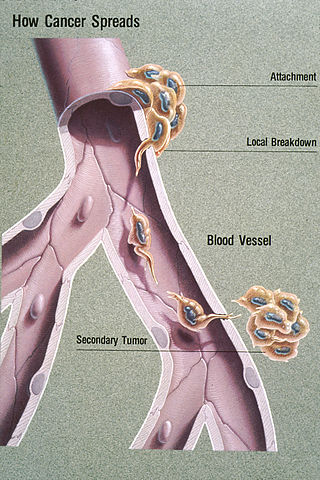
Metastasis is a pathogenic agent's spread from an initial or primary site to a different or secondary site within the host's body; the term is typically used when referring to metastasis by a cancerous tumor. The newly pathological sites, then, are metastases (mets). It is generally distinguished from cancer invasion, which is the direct extension and penetration by cancer cells into neighboring tissues.

Bladder cancer is any of several types of cancer arising from the tissues of the urinary bladder. Symptoms include blood in the urine, pain with urination, and low back pain. It is caused when epithelial cells that line the bladder become malignant.

Melanoma, also redundantly known as malignant melanoma, is a type of cancer that develops from the pigment-producing cells known as melanocytes. Melanomas typically occur in the skin, but may rarely occur in the mouth, intestines, or eye. In women, they most commonly occur on the legs, while in men, they most commonly occur on the back. About 25% of melanomas develop from moles. Changes in a mole that can indicate melanoma include an increase in size, irregular edges, change in color, itchiness, or skin breakdown.
Cancer staging is the process of determining the extent to which a cancer has grown and spread. A number from I to IV is assigned, with I being an isolated cancer and IV being a cancer that has metastasized and spread from its origin. The stage generally takes into account the size of a tumor, whether it has invaded adjacent organs, how many regional (nearby) lymph nodes it has spread to, and whether it has appeared in more distant locations (metastasized).
This is a list of terms related to oncology. The original source for this list was the US National Cancer Institute's public domain Dictionary of Cancer Terms.

Lymphadenectomy, or lymph node dissection, is the surgical removal of one or more groups of lymph nodes. It is almost always performed as part of the surgical management of cancer. In a regional lymph node dissection, some of the lymph nodes in the tumor area are removed; in a radical lymph node dissection, most or all of the lymph nodes in the tumor area are removed.

Lumpectomy is a surgical removal of a discrete portion or "lump" of breast tissue, usually in the treatment of a malignant tumor or breast cancer. It is considered a viable breast conservation therapy, as the amount of tissue removed is limited compared to a full-breast mastectomy, and thus may have physical and emotional advantages over more disfiguring treatment. Sometimes a lumpectomy may be used to either confirm or rule out that cancer has actually been detected. A lumpectomy is usually recommended to patients whose cancer has been detected early and who do not have enlarged tumors. Although a lumpectomy is used to allow for most of the breast to remain intact, the procedure may result in adverse affects that can include sensitivity and result in scar tissue, pain, and possible disfiguration of the breast if the lump taken out is significant. According to National Comprehensive Cancer Network guidelines, lumpectomy may be performed for ductal carcinoma in situ (DCIS), invasive ductal carcinoma, or other conditions.

Invasive carcinoma of no special type (NST) is also referred to as invasive ductal carcinoma or infiltrating ductal carcinoma(IDC) and invasive ductal carcinoma, not otherwise specified (NOS). Each of these terms represents to the same disease entity, but for international audiences this article will use invasive carcinoma NST because it is the preferred term of the World Health Organization (WHO).
A micrometastasis is a small collection of cancer cells that has been shed from the original tumor and spread to another part of the body through the lymphovascular system. Micrometastases are too few, in size and quantity, to be picked up in a screening or diagnostic test, and therefore cannot be seen with imaging tests such as a mammogram, MRI, ultrasound, PET, or CT scans. These migrant cancer cells may group together to form a second tumor, which is so small that it can only be seen under a microscope. Approximately ninety percent of people who die from cancer die from metastatic disease, since these cells are so challenging to detect. It is important for these cancer cells to be treated immediately after discovery, in order to prevent the relapse and the likely death of the patient.
Breast cancer management takes different approaches depending on physical and biological characteristics of the disease, as well as the age, over-all health and personal preferences of the patient. Treatment types can be classified into local therapy and systemic treatment. Local therapy is most efficacious in early stage breast cancer, while systemic therapy is generally justified in advanced and metastatic disease, or in diseases with specific phenotypes.
Breast-conserving surgery refers to an operation that aims to remove breast cancer while avoiding a mastectomy. Different forms of this operation include: lumpectomy (tylectomy), wide local excision, segmental resection, and quadrantectomy. Breast-conserving surgery has been increasingly accepted as an alternative to mastectomy in specific patients, as it provides tumor removal while maintaining an acceptable cosmetic outcome. This page reviews the history of this operation, important considerations in decision making and patient selection, and the emerging field of oncoplastic breast conservation surgery.
Uschi Keszler's Pennies in Action Cancer Research Fund, holding a full 501(c)(3) non-profit foundation status, exists to support research for breast cancer curative programs, including preventative vaccines and other biological therapies that do not damage the immune system.

Male breast cancer (MBC) is a cancer in males that originates in their breasts. Males account for less than 1% of new breast cancers with about 20,000 new cases being diagnosed worldwide every year. Its incidence rates in males vs. females are, respectively, 0.4 and 66.7 per 100,000 person-years. The worldwide incidences of male as well as female breast cancers have been increasing over the last few decades. Currently, one of every 800 men are estimated to develop this cancer during their lifetimes.
Indocyanine green (ICG) is a cyanine dye used in medical diagnostics. It is used for determining cardiac output, hepatic function, liver and gastric blood flow, and for ophthalmic and cerebral angiography. It has a peak spectral absorption at about 800 nm. These infrared frequencies penetrate retinal layers, allowing ICG angiography to image deeper patterns of circulation than fluorescein angiography. ICG binds tightly to plasma proteins and becomes confined to the vascular system. ICG has a half-life of 150 to 180 seconds and is removed from circulation exclusively by the liver to bile.

A gamma probe is a handheld device containing a scintillation counter, for intraoperative use following injection of a radionuclide, to locate sentinel lymph nodes by their radioactivity. It is used primarily for sentinel lymph node mapping and parathyroid surgery. Gamma probes are also used for RSL, to locate small and non-palpable breast lesions.
Souzan El-Eid is a breast surgical oncologist at Comprehensive Cancer Centers of Nevada (CCCN), and serves as the medical director of the Breast Care Center at Summerlin Hospital, cancer liaison physician for the cancer program and co-chair of the Breast Tumor Board at Summerlin Hospital. She is also the president elect for Clark County Medical Society. She is an Adjunct Associate Professor of General Surgery at Touro University Nevada and has served as principal investigator for several clinical research studies. She is the first breast surgeon in Las Vegas certified in both ultrasound and stereotactic breast biopsies.
Prognostic markers are biomarkers used to measure the progress of a disease in the patient sample. Prognostic markers are useful to stratify the patients into groups, guiding towards precise medicine discovery. The widely used prognostic markers in cancers include stage, size, grade, node and metastasis. In addition to these common markers, there are prognostic markers specific to different cancer types. For example estrogen level, progesterone and HER2 are markers specific to breast cancer patients. There is evidence showing that genes behaving as tumor suppressors or carcinogens could act as prognostic markers due to altered gene expression or mutation. Besides genetic biomarkers, there are also biomarkers that are detected in plasma or body fluid which can be metabolic or protein biomarkers.
Anne Louise Rosenberg is an American surgical oncologist retired from practice in Cherry Hill, New Jersey.

Armando Elario Giuliano is a surgical oncologist, surgeon scientist and medical professor in Los Angeles, California, United States of America. He is the Linda and Jim Lippman Chair in Surgical Oncology and co-director of Saul and Joyce Brandman Breast Center at Cedars-Sinai Medical Center, Los Angeles.
CP-GEP is a non-invasive prediction model for cutaneous melanoma patients that combines clinicopathologic (CP) variables with gene expression profiling (GEP). CP-GEP is able to identify cutaneous melanoma patients at low-risk for nodal metastasis who may forgo the sentinel lymph node biopsy (SLNB) procedure. The CP-GEP model was developed by the Mayo Clinic and SkylineDx BV, and it has been clinically validated in multiple studies.


