Related Research Articles
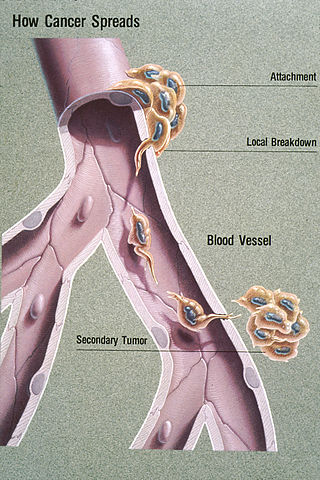
Metastasis is a pathogenic agent's spread from an initial or primary site to a different or secondary site within the host's body; the term is typically used when referring to metastasis by a cancerous tumor. The newly pathological sites, then, are metastases (mets). It is generally distinguished from cancer invasion, which is the direct extension and penetration by cancer cells into neighboring tissues.
Smegma is a combination of shed skin cells, skin oils, and moisture. It occurs in both male and female mammalian genitalia. In females, it collects around the clitoris and in the folds of the labia minora; in males, smegma collects under the foreskin.

Bladder cancer is any of several types of cancer arising from the tissues of the urinary bladder. Symptoms include blood in the urine, pain with urination, and low back pain. It is caused when epithelial cells that line the bladder become malignant.

Paraphimosis is an uncommon medical condition in which the foreskin of a penis becomes trapped behind the glans penis, and cannot be reduced. If this condition persists for several hours or there is any sign of a lack of blood flow, paraphimosis should be treated as a medical emergency, as it can result in gangrene.

Phimosis is a condition in which the foreskin of the penis cannot stretch to allow it to be pulled back past the glans. A balloon-like swelling under the foreskin may occur with urination. In teenagers and adults, it may result in pain during an erection, but is otherwise not painful. Those affected are at greater risk of inflammation of the glans, known as balanitis, and other complications.

Balanitis is inflammation of the glans penis. When the foreskin is also affected, the proper term is balanoposthitis. Balanitis on boys still in diapers must be distinguished from redness caused by ammoniacal dermatitis. The word balanitis is from the Greek βάλανοςbalanos, literally meaning 'acorn', used because of the similarity in shape to the glans penis.

Anal cancer is a cancer which arises from the anus, the distal opening of the gastrointestinal tract. Symptoms may include bleeding from the anus or a lump near the anus. Other symptoms may include pain, itchiness, or discharge from the anus. A change in bowel movements may also occur.

Lichen sclerosus (LS) is a chronic, inflammatory skin disease of unknown cause which can affect any body part of any person but has a strong preference for the genitals and is also known as balanitis xerotica obliterans (BXO) when it affects the penis. Lichen sclerosus is not contagious. There is a well-documented increase of skin cancer risk in LS, potentially improvable with treatment. LS in adult age women is normally incurable, but improvable with treatment, and often gets progressively worse if not treated properly. Most males with mild or intermediate disease restricted to foreskin or glans can be cured by either medical or surgical treatment.

Invasive carcinoma of no special type, invasive breast carcinoma of no special type (IBC-NST), invasive ductal carcinoma (IDC), infiltrating ductal carcinoma (IDC) or invasive ductal carcinoma, not otherwise specified (NOS) is a disease. For international audiences this article will use "invasive carcinoma NST" because it is the preferred term of the World Health Organization (WHO).
The uterine sarcomas form a group of malignant tumors that arises from the smooth muscle or connective tissue of the uterus. They can be difficult to detect, as symptoms are common to other uterine conditions and no specific screening test has been developed. This presents an issue for treatment, as the cancer spreads quickly.

Verrucous carcinoma (VC) is an uncommon variant of squamous cell carcinoma. This form of cancer is often seen in those who chew tobacco or use snuff orally, so much so that it is sometimes referred to as "Snuff dipper's cancer".

Vulvar cancer is a cancer of the vulva, the outer portion of the female genitals. It most commonly affects the labia majora. Less often, the labia minora, clitoris, or Bartholin's glands are affected. Symptoms include a lump, itchiness, changes in the skin, or bleeding from the vulva.

Urethral cancer is a rare cancer originating from the urethra. The disease has been classified by the TNM staging system and the World Health Organization.

Circumcision is a procedure that removes the foreskin from the human penis. In the most common form of the operation, the foreskin is extended with forceps, then a circumcision device may be placed, after which the foreskin is excised. Topical or locally injected anesthesia is generally used to reduce pain and physiologic stress. Circumcision is generally electively performed, most commonly done as a form of preventive healthcare, as a religious obligation, or as a cultural practice. It is also an option for cases of phimosis, other pathologies that do not resolve with other treatments, and chronic urinary tract infections (UTIs). The procedure is contraindicated in cases of certain genital structure abnormalities or poor general health.
Vaginal cancer is an extraordinarily rare form of cancer that develops in the tissue of the vagina. Primary vaginal cancer originates from the vaginal tissue – most frequently squamous cell carcinoma, but primary vaginal adenocarcinoma, sarcoma, and melanoma have also been reported – while secondary vaginal cancer involves the metastasis of a cancer that originated in a different part of the body. Secondary vaginal cancer is more common. Signs of vaginal cancer may include abnormal vaginal bleeding, dysuria, tenesmus, or pelvic pain, though as many as 20% of women diagnosed with vaginal cancer are asymptomatic at the time of diagnosis. Vaginal cancer occurs more frequently in women over age 50, and the mean age of diagnosis of vaginal cancer is 60 years. It often can be cured if found and treated in early stages. Surgery alone or surgery combined with pelvic radiation is typically used to treat vaginal cancer.
Pseudoepitheliomatous keratotic and micaceous balanitis, (PKMB) is a cutaneous condition characterized by skin lesions on the glans penis that are wart-like with scaling. It can present as a cutaneous horn. PKMB is usually asymptomatic, with occasional irritation, burning sensation, fissuring, or maceration.

A dorsal slit is a single incision along the upper length of the foreskin from the tip to the corona, exposing the glans without removing any tissue. An ancient practice, it has been a traditional custom among a number of peoples, particularly Filipinos and Pacific Islanders, probably for thousands of years.

In male human anatomy, the foreskin, also known as the prepuce, is the double-layered fold of skin, mucosal and muscular tissue at the distal end of the human penis that covers the glans and the urinary meatus. The foreskin is attached to the glans by an elastic band of tissue, known as the frenulum. The outer skin of the foreskin meets with the inner preputial mucosa at the area of the mucocutaneous junction. The foreskin is mobile, fairly stretchable and sustains the glans in a moist environment. Except for humans, a similar structure known as a penile sheath appears in the male sexual organs of all primates and the vast majority of mammals.
Skin cancer, or neoplasia, is the most common type of cancer diagnosed in horses, accounting for 45 to 80% of all cancers diagnosed. Sarcoids are the most common type of skin neoplasm and are the most common type of cancer overall in horses. Squamous-cell carcinoma is the second-most prevalent skin cancer, followed by melanoma. Squamous-cell carcinoma and melanoma usually occur in horses greater than 9-years-old, while sarcoids commonly affect horses 3 to 6 years old. Surgical biopsy is the method of choice for diagnosis of most equine skin cancers, but is contraindicated for cases of sarcoids. Prognosis and treatment effectiveness varies based on type of cancer, degree of local tissue destruction, evidence of spread to other organs (metastasis) and location of the tumor. Not all cancers metastasize and some can be cured or mitigated by surgical removal of the cancerous tissue or through use of chemotherapeutic drugs.
Carcinoma of the tonsil is a type of squamous cell carcinoma. The tonsil is the most common site of squamous cell carcinoma in the oropharynx. It comprises 23.1% of all malignancies of the oropharynx. The tumors frequently present at advanced stages, and around 70% of patients present with metastasis to the cervical lymph nodes. . The most reported complaints include sore throat, otalgia or dysphagia. Some patients may complain of feeling the presence of a lump in the throat. Approximately 20% patients present with a node in the neck as the only symptom.
References
- 1 2 3 "Penile Cancer Factsheet" (PDF). Global Cancer Observatory. Retrieved 7 January 2022.
- ↑ "Signs and Symptoms of Penile Cancer | Signs Of Penile Cancer". www.cancer.org. Retrieved 2019-12-18.
- ↑ Sumedia-Online. "EAU Guidelines: Penile Cancer". Uroweb. Retrieved 2019-12-18.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 Bleeker MC, Heideman DA, Snijders PJ, Horenblas S, Dillner J, Meijer CJ (April 2009). "Penile cancer: epidemiology, pathogenesis and prevention". World Journal of Urology. 27 (2): 141–50. doi:10.1007/s00345-008-0302-z. PMID 18607597. S2CID 25742226.
- 1 2 Turner, Bruce; Drudge-Coates, Lawrence; Henderson, Sarah (2013-03-20). "Penile cancer: diagnosis, clinical features and management". Nursing Standard. 27 (29): 50–57. doi:10.7748/ns2013.03.27.29.50.e6135. ISSN 0029-6570. PMID 23634501.
- 1 2 "Signs and Symptoms of Penile Cancer | Signs Of Penile Cancer". www.cancer.org. Retrieved 2020-12-08.
- 1 2 3 4 5 6 7 8 9 "What Are the Risk Factors for Penile Cancer?". www.cancer.org. Retrieved 2 April 2018.
- ↑ Bleeker MC, Heideman DL, Snijders PJ, Horenblas S, Meijer CJ (2011). "Epidemiology and Etiology of Penile Cancer". Textbook of Penile Cancer. pp. 1–11. doi:10.1007/978-1-84882-879-7_1. ISBN 978-1-84882-878-0.
- 1 2 3 4 5 6 7 Pow-Sang MR, Ferreira U, Pow-Sang JM, Nardi AC, Destefano V (August 2010). "Epidemiology and natural history of penile cancer". Urology. 76 (2 Suppl 1): S2-6. doi:10.1016/j.urology.2010.03.003. PMID 20691882.
- ↑ "Penile Cancer". National Cancer Institute. 1980-01-01. Retrieved 2 April 2018.
- ↑ https://www.cdc.gov/cancer/hpv/statistics/penile.htm HPV-Associated Penile Cancer Rates by Race and Ethnicity] Centers for Disease Control and Prevention
- ↑ de Bravo BF, DeSoto M, Seu K (April 2009). "HPV: Q&A". Cancer Prevention and Treatment Fund. Retrieved August 13, 2013.
- 1 2 "Risks and causes - Penile cancer - Cancer Research UK". cancerhelp.cancerresearchuk.org. 2017-08-30. Retrieved 2 April 2018.
- 1 2 3 4 5 6 7 Minhas S, Manseck A, Watya S, Hegarty PK (August 2010). "Penile cancer--prevention and premalignant conditions". Urology. 76 (2 Suppl 1): S24-35. doi:10.1016/j.urology.2010.04.007. PMID 20691883.
- ↑ Reis AA, Paula LB, Paula AA, Saddi VA, Cruz AD (June 2010). "[Clinico-epidemiological aspects associated with penile cancer]". Ciencia & Saude Coletiva (in Portuguese). 15 (Suppl 1): 1105–11. doi: 10.1590/s1413-81232010000700018 . PMID 20640268.
- ↑ Morris BJ, Gray RH, Castellsague X, Bosch FX, Halperin DT, Waskett JH, Hankins CA (2011). "The Strong Protective Effect of Circumcision against Cancer of the Penis". Advances in Urology. 2011: 812368. doi: 10.1155/2011/812368 . PMC 3113366 . PMID 21687572.
- ↑ PubMed Health PubMed, Last Reviewed: September 16, 2011
- ↑ "Symptoms of penile cancer - Penile cancer - Cancer Research UK". cancerhelp.cancerresearchuk.org. 2017-08-30. Retrieved 2 April 2018.
- 1 2 Larke NL, Thomas SL, dos Santos Silva I, Weiss HA (August 2011). "Male circumcision and penile cancer: a systematic review and meta-analysis". Cancer Causes & Control. 22 (8): 1097–110. doi:10.1007/s10552-011-9785-9. PMC 3139859 . PMID 21695385.
- ↑ Micali G, Nasca MR, Innocenzi D, Schwartz RA (March 2006). "Penile cancer". Journal of the American Academy of Dermatology. 54 (3): 369–91, quiz 391–4. doi:10.1016/j.jaad.2005.05.007. PMID 16488287.
- ↑ Canete-Portillo S, Velazquez EF, Kristiansen G, Egevad L, Grignon D, Chaux A, Cubilla AL (July 2020). "Report From the International Society of Urological Pathology (ISUP) Consultation Conference on Molecular Pathology of Urogenital Cancers V: Recommendations on the Use of Immunohistochemical and Molecular Biomarkers in Penile Cancer". The American Journal of Surgical Pathology. 44 (7): e80–e86. doi:10.1097/PAS.0000000000001477. PMID 32235153. S2CID 214766446.
- ↑ "Penile Cancer". The Lecturio Medical Concept Library. Retrieved 3 October 2021.
- 1 2 3 4 "Stage Information for Penile Cancer". National Cancer Institute. 1980-01-01. Retrieved 3 November 2013.
- 1 2 3 Shabbir M, Barod R, Hegarty PK, Minhas S (2013). "Primary prevention and vaccination for penile cancer". Ther Adv Urol. 5 (3): 161–169. doi:10.1177/1756287212465456. PMC 3655354 . PMID 23730331.
- ↑ de Souza KW, dos Reis PE, Gomes IP, de Carvalho EC (March 2011). "[Prevention strategies for testicular and penile cancer: an integrative review]". Revista da Escola de Enfermagem da USP (in Portuguese). 45 (1): 277–82. doi: 10.1590/s0080-62342011000100039 . PMID 21445520.
- ↑ Engelsgjerd JS, LaGrange CA (2020). Penile Cancer. Treasure Island (FL): StatPearls Publishing. PMID 29763105 . Retrieved 2020-12-07.
{{cite book}}:|work=ignored (help) - ↑ Hakenberg OW, Dräger DL, Erbersdobler A, Naumann CM, Jünemann KP, Protzel C (September 2018). "The Diagnosis and Treatment of Penile Cancer". Deutsches Ärzteblatt International. 115 (39): 646–652. doi:10.3238/arztebl.2018.0646. PMC 6224543 . PMID 30375327.
- ↑ The American Cancer Society: Penile Cancer: What is penile cancer? American Cancer Society, Last revised: January 8, 2012
- ↑ The Official Website of the Royal Australasian College of Physicians, Published September 2010
- ↑ Frisch M, Friis S, Kjaer SK, Melbye M (December 1995). "Falling incidence of penis cancer in an uncircumcised population (Denmark 1943-90)". BMJ (Clinical Research Ed.). 311 (7018): 1471. doi:10.1136/bmj.311.7018.1471. PMC 2543732 . PMID 8520335.
- ↑ The American Cancer Society: Penile Cancer: What are the key statistics about penile cancer American Cancer Society, Last revised: January 18, 2012
- ↑ Cold CJ, Storms MR, Van Howe RS (April 1997). "Carcinoma in situ of the penis in a 76-year-old circumcised man". The Journal of Family Practice. 44 (4): 407–10. PMID 9108839.