External links
| Pregnancy |
| ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Labor | |||||||||||||||||
| Puerperal | |||||||||||||||||
| Other | |||||||||||||||||
| International | |
|---|---|
| National | |
| Postterm pregnancy | |
|---|---|
| Other names | Postterm, postmaturity, prolonged pregnancy, post-dates pregnancy, postmature birth |
| Specialty | Obstetrics |
Postterm pregnancy is when a woman has not yet delivered her baby after 42 weeks of gestation, two weeks beyond the typical 40-week duration of pregnancy. [1] Postmature births carry risks for both the mother and the baby, including fetal malnutrition, meconium aspiration syndrome, and stillbirths. [2] After the 42nd week of gestation, the placenta, which supplies the baby with nutrients and oxygen from the mother, starts aging and will eventually fail. Postterm pregnancy is a reason to induce labor. [3]
The management of labor and delivery may vary depending on the gestational age. It is common to encounter the following terms when describing different time periods of pregnancy. [4]
Besides postterm pregnancy, other terminologies have been used to describe the same condition (≥ 42w+0d), such as prolonged pregnancy, postdates, and postdatism. [6] However, these terminologies are less commonly used to avoid confusion. [7]
Postterm pregnancy should not be confused with postmaturity, postmaturity syndrome, or dysmaturity. These terms describe the neonatal condition that may be caused by postterm pregnancy instead of the duration of pregnancy. [6]
Because postterm pregnancy is a condition solely based on gestational age, there are no confirming physical signs or symptoms. While it is difficult to determine gestational age physically, infants that are born postterm may be associated with a physical condition called postmaturity. The most common symptoms for this condition are dry skin, overgrown nails, creases on the baby's palms and soles of their feet, minimal fat, abundant hair on their head, and either a brown, green, or yellow discoloration of their skin. Doctors diagnose postmature birth based on the baby's physical appearance and the length of the mother's pregnancy. [8] However, some postmature babies may show no or few signs of postmaturity.
A 2019 randomized control trial of induced labor at 42 or 43 weeks was terminated early due to statistical evidence of "significantly increased risk for women induced at the start of week 43". The study implies clinical guidelines for induction of labor no later than at 41 gestational weeks. [22]
The causes of post-term births are unknown, but postmature births are more likely when the mother has experienced a previous postmature birth. Due dates are easily miscalculated when the mother is unsure of her last menstrual period. When there is a miscalculation, the baby could be delivered before or after the expected due date. [23] Postmature births can also be attributed to irregular menstrual cycles. When the menstrual period is irregular it is difficult to judge the moment of ovulation and subsequent fertilization and pregnancy. Some postmature pregnancies may not be postmature in reality due to the uncertainty of mother's last menstrual period. [3] However, in most countries where gestation is measured by ultrasound scan technology, this is less likely.[ citation needed ]
Once a pregnancy is diagnosed postterm, usually at or greater than 42 weeks of gestational age, the mother should be offered additional monitoring as this can provide valuable clues that the fetal health is being maintained. [24]
Regular movements of the fetus is the best sign indicating that it is still in good health. The mother should keep a "kick-chart" to record the movements of her fetus. If there is a reduction in the number of movements it could indicate placental deterioration. [25] [ dead link ]
Doppler fetal monitor is a hand-held device that is routinely used in prenatal care. When it is used correctly, it can quickly measure the fetal heart rate. The baseline of fetal heart rate is typically between 110 and 160 beats per minute. [26]
Doppler flow study is a type of ultrasound that measures the amount of blood flowing in and out of the placenta. [13] The ultrasound machine can also detect the direction of blood flow and display it in red or blue. Usually, a red color indicates a flow toward the ultrasound transducer, while blue indicates a flow away from the transducer. Based on the display, doctors can evaluate blood flow to the umbilical arteries, umbilical veins, or other organs such as heart and brain. [27]
Nonstress test (NST) is a type of electronic fetal monitoring that uses a cardiotocograph to monitor fetal heartbeat, fetal movement and mother's contraction. NST is typically monitored for at least 20 minutes. Signs of a reactive (normal) NST include a baseline fetal heart rate (FHR) between 110 and 160 beats per minute (bpm) and 2 accelerations of FHR of at least 15 bpm above baseline for over 15 seconds. Vibroacoustic stimulation and longer monitoring may be needed if NST is non-reactive. [28]
A biophysical profile is a noninvasive procedure that uses the ultrasound to evaluate the fetal health based on NST and four ultrasound parameters: fetal movement, fetal breathing, fetal muscle tone, and the amount of amniotic fluid surrounding the fetus. A score of 2 points is given for each category that meets the criteria or 0 points if the criteria are not met (no 1 point). Sometimes, the NST is omitted, making the highest score 8/8 instead of 10/10. Generally, a score of 8/10 or 10/10 is considered a normal test result, unless 0 points is given for amniotic fluid. A score of 6/10 with normal amniotic fluid is considered equivocal, and a repeated test within 24 hours may be needed. A score of 4/10 or less is considered abnormal, and delivery may be indicated. [29] Low amniotic fluid can cause pinching umbilical cord, decreasing blood flow to the fetus. Therefore, a score of 0 points for amniotic fluid may indicate the fetus is at risk. [30]
A woman who has reached 42 weeks of pregnancy is likely to be offered induction of labour. Alternatively, she can choose expectant management, that is, she waits for the natural onset of labour. Women opting for expectant management may also choose to carry on with additional monitoring of their baby, with regular CTG, ultrasound, and biophysical profile. Risks of expectant management vary between studies. [31]
In many places in the World, according to the World Health Organization and others, such services are rudimentary or not available, and deserve improvement.
Inducing labor artificially starts the labor process by using medication and other techniques. Labor is usually only induced if there is potential danger on the mother or child. [32] There are several reasons for labor induction; the mother's water breaks, and contractions have not started, the child is postmature, the mother has diabetes or high blood pressure, or there is not enough amniotic fluid around the baby. [33] Labor induction is not always the best choice because it has its own risks. Sometimes mothers will request to be induced for reasons that are not medical. This is called an elective induction. Doctors try to avoid inducing labor unless it is completely necessary. [32]
There are four common methods of starting contractions. The four most common are stripping the membranes, breaking the mother's water, giving the hormone prostaglandin, and giving the synthetic hormone pitocin. Stripping the membranes does not work for all women, but can for most. [34] [35] A doctor inserts a finger into the mother's cervix and moves it around to separate the membrane connecting the amniotic sac, which houses the baby, from the walls of the uterus. Once this membrane is stripped, the hormone prostaglandin is naturally released into the mother's body and initiates contractions. [32] Most of the time doing this only once will not immediately start labor. It may have to be done several times before the stimulant hormone is released, and contractions start. [36] The next method is breaking the mother's water, which is also referred to as an amniotomy. The doctor uses a plastic hook to break the membrane and rupture the amniotic sac. Within a few hours labor usually begins. Giving the hormone prostaglandin ripens the cervix, meaning the cervix softens, thins out, or dilates. The drug Cervidil is administered by mouth in tablet form or in gel form as an insert. This is most often done in the hospital overnight. The hormone oxytocin is usually given in the synthetic form of Pitocin. It is administered through an IV throughout the labor process. This hormone stimulates contractions. Pitocin is also used to "restart" labor when it is lagging.[ citation needed ]
The use of misoprostol is also allowed, but close monitoring of the mother is required.[ citation needed ]
Prevalence of postterm pregnancy may vary between countries due to different population characteristics or medical management. Factors include number of first-time pregnancies, genetic predisposition, timing of ultrasound assessment, and Caesarean section rates, etc. The incidence is approximately 7%. [6] Postterm pregnancy occurs in 0.4% of pregnancies approximately in the United States according to birth certificate data. [37]
{{cite book}}: CS1 maint: multiple names: authors list (link)| Pregnancy |
| ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Labor | |||||||||||||||||
| Puerperal | |||||||||||||||||
| Other | |||||||||||||||||
| International | |
|---|---|
| National | |

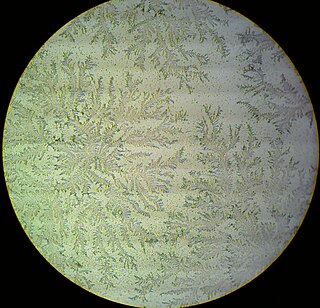
Amniocentesis is a medical procedure used primarily in the prenatal diagnosis of genetic conditions. It has other uses such as in the assessment of infection and fetal lung maturity. Prenatal diagnostic testing, which includes amniocentesis, is necessary to conclusively diagnose the majority of genetic disorders, with amniocentesis being the gold-standard procedure after 15 weeks' gestation.
The amniotic sac, also called the bag of waters or the membranes, is the sac in which the embryo and later fetus develops in amniotes. It is a thin but tough transparent pair of membranes that hold a developing embryo until shortly before birth. The inner of these membranes, the amnion, encloses the amniotic cavity, containing the amniotic fluid and the embryo. The outer membrane, the chorion, contains the amnion and is part of the placenta. On the outer side, the amniotic sac is connected to the yolk sac, the allantois, and via the umbilical cord, the placenta.
Fetal distress, also known as non-reassuring fetal status, is a condition during pregnancy or labor in which the fetus shows signs of inadequate oxygenation. Due to its imprecision, the term "fetal distress" has fallen out of use in American obstetrics. The term "non-reassuring fetal status" has largely replaced it. It is characterized by changes in fetal movement, growth, heart rate, and presence of meconium stained fluid.

External cephalic version (ECV) is a process by which a breech baby can sometimes be turned from buttocks or foot first to head first. It is a manual procedure that is recommended by national guidelines for breech presentation of a pregnancy with a single baby, in order to enable vaginal delivery. It is usually performed late in pregnancy, that is, after 36 gestational weeks, preferably 37 weeks, and can even be performed in the early stages of childbirth.
Oligohydramnios is a medical condition in pregnancy characterized by a deficiency of amniotic fluid, the fluid that surrounds the fetus in the abdomen, in the amniotic sac. It is typically diagnosed by ultrasound when the amniotic fluid index (AFI) measures less than 5 cm or when the single deepest pocket (SDP) of amniotic fluid measures less than 2 cm. Amniotic fluid is necessary to allow for normal fetal movement, lung development, and cushioning from uterine compression. Low amniotic fluid can be attributed to a maternal, fetal, placental or idiopathic cause and can result in poor fetal outcomes including death. The prognosis of the fetus is dependent on the etiology, gestational age at diagnosis, and the severity of the oligohydramnios.
Labor induction is the process or treatment that stimulates childbirth and delivery. Inducing (starting) labor can be accomplished with pharmaceutical or non-pharmaceutical methods. In Western countries, it is estimated that one-quarter of pregnant women have their labor medically induced with drug treatment. Inductions are most often performed either with prostaglandin drug treatment alone, or with a combination of prostaglandin and intravenous oxytocin treatment.
Rupture of membranes (ROM) or amniorrhexis is a term used during pregnancy to describe a rupture of the amniotic sac. Normally, it occurs spontaneously at full term either during or at the beginning of labor. Rupture of the membranes is known colloquially as "breaking (one's) water," especially when induced rather than spontaneous, or as one's "water breaking". A premature rupture of membranes (PROM) is a rupture of the amnion that occurs at full term and prior to the onset of labor. In cases of PROM, options include expectant management without intervention, or interventions such as oxytocin or other methods of labor induction, and both are usually accompanied by close monitoring of maternal and fetal health. Preterm premature rupture of membranes (PPROM) is when water breaks both before the onset of labor and before the pregnancy's 37 week gestation. In the United States, more than 120,000 pregnancies per year are affected by a premature rupture of membranes, which is the cause of about one third of preterm deliveries.
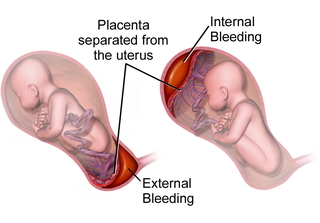
Placental abruption is when the placenta separates early from the uterus, in other words separates before childbirth. It occurs most commonly around 25 weeks of pregnancy. Symptoms may include vaginal bleeding, lower abdominal pain, and dangerously low blood pressure. Complications for the mother can include disseminated intravascular coagulopathy and kidney failure. Complications for the baby can include fetal distress, low birthweight, preterm delivery, and stillbirth.
Prelabor rupture of membranes (PROM), previously known as premature rupture of membranes, is breakage of the amniotic sac before the onset of labor. Women usually experience a painless gush or a steady leakage of fluid from the vagina. Complications in the baby may include premature birth, cord compression, and infection. Complications in the mother may include placental abruption and postpartum endometritis.

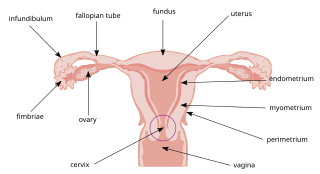
An abdominal pregnancy is a rare type of ectopic pregnancy where the embryo or fetus is growing and developing outside the uterus, in the abdomen, and not in a fallopian tube, an ovary, or the broad ligament.
Cervical effacement or cervical ripening refers to the thinning and shortening of the cervix. This process occurs during labor to prepare the cervix for dilation to allow the fetus to pass through the vagina. While this a normal, physiological process that occurs at the later end of pregnancy, it can also be induced through medications and procedures.
An asynclitic birth or asynclitism are terms used in obstetrics to refer to childbirth in which there is malposition of the head of the fetus in the uterus, relative to the birth canal. Asynclitic presentation is different from a shoulder presentation, in which the shoulder is presenting first. Many babies enter the pelvis in an asynclitic presentation, and most asynclitism corrects spontaneously as part of the normal birthing process.
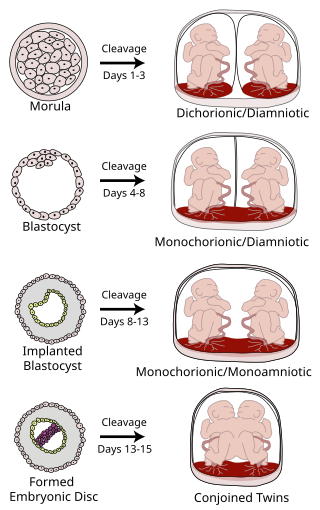
Monoamniotic twins are identical or semi-identical twins that share the same amniotic sac within their mother's uterus. Monoamniotic twins are always monochorionic and are usually termed Monoamniotic-Monochorionic twins. They share the placenta, but have two separate umbilical cords. Monoamniotic twins develop when an embryo does not split until after formation of the amniotic sac, at about 9–13 days after fertilization. Monoamniotic triplets or other monoamniotic multiples are possible, but extremely rare. Other obscure possibilities include multiples sets where monoamniotic twins are part of a larger gestation such as triplets, quadruplets, or more.
A uterotonic, also known as an oxytocic or ecbolic, is a type of medication used to induce contraction or greater tonicity of the uterus. Uterotonics are used both to induce labor and to reduce postpartum hemorrhage.
The following outline is provided as an overview of and topical guide to obstetrics:
Post-maturity syndrome refers to the condition of a baby born after a post-term pregnancy, first described by Stewart H. Clifford in 1954. Post-maturity refers to any baby born after 42 weeks gestation, or 294 days past the first day of the mother's last menstrual period. Less than 6 percent of all babies are born after this time. The syndrome develops in about 20% of human pregnancies continuing past the expected delivery date.

Circumvallate placenta is a rare condition affecting about 1-2% of pregnancies, in which the amnion and chorion fetal membranes essentially "double back" on the fetal side around the edges of the placenta. After delivery, a circumvallate placenta has a thick ring of membranes on its fetal surface. Circumvallate placenta is a placental morphological abnormality associated with increased fetal morbidity and mortality due to the restricted availability of nutrients and oxygen to the developing fetus.
Amnioinfusion is a method in which isotonic fluid is instilled into the uterine cavity.
Artificial rupture of membranes (AROM), also known as an amniotomy, is performed by a midwife or obstetrician and was once thought to be an effective means to induce or accelerate labor. The membranes can be ruptured using a specialized tool, such as an amnihook or amnicot, or they may be ruptured by the proceduralist's finger. The different techniques for artificial rupture of membranes have not been extensively compared in the literature. In one study comparing amnihook versus amnicot for artificial rupture of membranes, use of an amnicot was associated with fewer neonatal scalp lacerations.
Emergency childbirth is the precipitous birth of an infant in an unexpected setting. In planned childbirth, mothers choose the location and obstetric team ahead of time. Options range from delivering at home, at a hospital, a medical facility or a birthing center. Sometimes, birth can occur on the way to these facilities, without a healthcare team. The rates of unplanned childbirth are low. If the birth is imminent, emergency measures may be needed. Emergency services can be contacted for help in some countries.