
Mouthwash, mouth rinse, oral rinse, or mouth bath is a liquid which is held in the mouth passively or swirled around the mouth by contraction of the perioral muscles and/or movement of the head, and may be gargled, where the head is tilted back and the liquid bubbled at the back of the mouth.
Listerine is a brand of antiseptic mouthwash that is promoted with the slogan "Kills germs that cause bad breath". Named after Joseph Lister, who pioneered antiseptic surgery at the Glasgow Royal Infirmary in Scotland, Listerine was developed in 1879 by Joseph Lawrence, a chemist in St. Louis, Missouri.
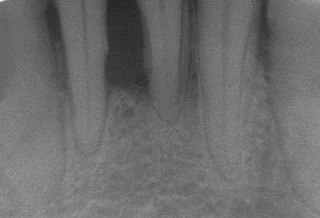
Periodontal disease, also known as gum disease, is a set of inflammatory conditions affecting the tissues surrounding the teeth. In its early stage, called gingivitis, the gums become swollen and red and may bleed. It is considered the main cause of tooth loss for adults worldwide. In its more serious form, called periodontitis, the gums can pull away from the tooth, bone can be lost, and the teeth may loosen or fall out. Halitosis may also occur.

Necrotizing gingivitis (NG) is a common, non-contagious infection of the gums with sudden onset. The main features are painful, bleeding gums, and ulceration of interdental papillae. This disease, along with necrotizing periodontitis (NP) and necrotizing stomatitis, is classified as a necrotizing periodontal disease, one of the three general types of gum disease caused by inflammation of the gums (periodontitis).

Toothaches, also known as dental pain or tooth pain, is pain in the teeth or their supporting structures, caused by dental diseases or pain referred to the teeth by non-dental diseases. When severe it may impact sleep, eating, and other daily activities.

Tonsil stones, also known as tonsilloliths, are mineralizations of debris within the crevices of the tonsils. When not mineralized, the presence of debris is known as chronic caseous tonsillitis (CCT). Symptoms may include bad breath, foreign body sensation, sore throat, pain or discomfort with swallowing, and cough. Generally there is no pain, though there may be the feeling of something present. The presence of tonsil stones may be otherwise undetectable; however, some people have reported seeing white material in the rear of their throat.

Xerostomia, also known as dry mouth, is a subjective complaint of dryness in the mouth, which may be associated with a change in the composition of saliva, or reduced salivary flow, or have no identifiable cause.

Trimethylaminuria (TMAU), also known as fish odor syndrome or fish malodor syndrome, is a rare metabolic disorder that causes a defect in the normal production of an enzyme named flavin-containing monooxygenase 3 (FMO3). When FMO3 is not working correctly or if not enough enzyme is produced, the body loses the ability to properly convert the fishy-smelling chemical trimethylamine (TMA) from precursor compounds in food digestion into trimethylamine oxide (TMAO), through a process called N-oxidation.
Periodontology or periodontics is the specialty of dentistry that studies supporting structures of teeth, as well as diseases and conditions that affect them. The supporting tissues are known as the periodontium, which includes the gingiva (gums), alveolar bone, cementum, and the periodontal ligament. A periodontist is a dentist that specializes in the prevention, diagnosis and treatment of periodontal disease and in the placement of dental implants.
Dental plaque is a biofilm of microorganisms that grows on surfaces within the mouth. It is a sticky colorless deposit at first, but when it forms tartar, it is often brown or pale yellow. It is commonly found between the teeth, on the front of teeth, behind teeth, on chewing surfaces, along the gumline (supragingival), or below the gumline cervical margins (subgingival). Dental plaque is also known as microbial plaque, oral biofilm, dental biofilm, dental plaque biofilm or bacterial plaque biofilm. Bacterial plaque is one of the major causes for dental decay and gum disease. Interestingly, it has been observed that differences in the composition of dental plaque microbiota exist between men and women, particularly in the presence of periodontitis.

Pericoronitis is inflammation of the soft tissues surrounding the crown of a partially erupted tooth, including the gingiva (gums) and the dental follicle. The soft tissue covering a partially erupted tooth is known as an operculum, an area which can be difficult to access with normal oral hygiene methods. The hyponym operculitis technically refers to inflammation of the operculum alone.
Olfactory reference syndrome (ORS) is a psychiatric condition in which there is a persistent false belief and preoccupation with the idea of emitting abnormal body odors which the patient thinks are foul and offensive to other individuals. People with this condition often misinterpret others' behaviors, e.g. sniffing, touching their nose or opening a window, as being referential to an unpleasant body odor which in reality is non-existent and cannot be detected by other people.

Tooth brushing is the act of scrubbing teeth with a toothbrush equipped with toothpaste. Interdental cleaning can be useful with tooth brushing, and together these two activities are the primary means of cleaning teeth, one of the main aspects of oral hygiene. The recommended amount of time for tooth brushing is two minutes each time for two times a day.
A Halimeter is an instrument for measurement of the level of volatile sulfur compounds (VSCs) in the mouth.

Oral hygiene is the practice of keeping one's oral cavity clean and free of disease and other problems by regular brushing of the teeth and adopting good hygiene habits. It is important that oral hygiene be carried out on a regular basis to enable prevention of dental disease and bad breath. The most common types of dental disease are tooth decay and gum diseases, including gingivitis, and periodontitis.

A tongue cleaner is an oral hygiene device designed to clean the coating on the upper surface of the tongue. While there is tentative benefit from the use of a tongue cleaner it is insufficient to draw clear conclusions regarding bad breath.

Gingivitis is a non-destructive disease that causes inflammation of the gums; ulitis is an alternative term. The most common form of gingivitis, and the most common form of periodontal disease overall, is in response to bacterial biofilms that are attached to tooth surfaces, termed plaque-induced gingivitis. Most forms of gingivitis are plaque-induced.

Mel Rosenberg is a Canadian microbiologist best known for his research on the diagnosis and treatment of bad breath (halitosis).
Peri-implant mucositis is defined as an inflammatory lesion of the peri-implant mucosa in the absence of continuing marginal bone loss.

Tooth pathology is any condition of the teeth that can be congenital or acquired. Sometimes a congenital tooth disease is called a tooth abnormality. These are among the most common diseases in humans The prevention, diagnosis, treatment and rehabilitation of these diseases are the base to the dentistry profession, in which are dentists and dental hygienists, and its sub-specialties, such as oral medicine, oral and maxillofacial surgery, and endodontics. Tooth pathology is usually separated from other types of dental issues, including enamel hypoplasia and tooth wear.

