
Cholera is an infection of the small intestine by some strains of the bacterium Vibrio cholerae. Symptoms may range from none, to mild, to severe. The classic symptom is large amounts of watery diarrhea lasting a few days. Vomiting and muscle cramps may also occur. Diarrhea can be so severe that it leads within hours to severe dehydration and electrolyte imbalance. This may result in sunken eyes, cold skin, decreased skin elasticity, and wrinkling of the hands and feet. Dehydration can cause the skin to turn bluish. Symptoms start two hours to five days after exposure.

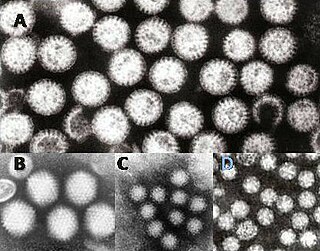
Rotaviruses are the most common cause of diarrhoeal disease among infants and young children. Nearly every child in the world is infected with a rotavirus at least once by the age of five. Immunity develops with each infection, so subsequent infections are less severe. Adults are rarely affected. Rotavirus is a genus of double-stranded RNA viruses in the family Reoviridae. There are nine species of the genus, referred to as A, B, C, D, F, G, H, I and J. Rotavirus A is the most common species, and these rotaviruses cause more than 90% of rotavirus infections in humans.

Giardiasis is a parasitic disease caused by Giardia duodenalis. Infected individuals who experience symptoms may have diarrhoea, abdominal pain, and weight loss. Less common symptoms include vomiting and blood in the stool. Symptoms usually begin one to three weeks after exposure and, without treatment, may last two to six weeks or longer.

Enteritis is inflammation of the small intestine. It is most commonly caused by food or drink contaminated with pathogenic microbes, such as Serratia, but may have other causes such as NSAIDs, radiation therapy as well as autoimmune conditions like coeliac disease. Symptoms include abdominal pain, cramping, diarrhoea, dehydration, and fever. Related diseases of the gastrointestinal system involve inflammation of the stomach and large intestine.

Malabsorption is a state arising from abnormality in absorption of food nutrients across the gastrointestinal (GI) tract. Impairment can be of single or multiple nutrients depending on the abnormality. This may lead to malnutrition and a variety of anaemias.
Gastroenteritis, also known as infectious diarrhea, is an inflammation of the gastrointestinal tract including the stomach and intestine. Symptoms may include diarrhea, vomiting, and abdominal pain. Fever, lack of energy, and dehydration may also occur. This typically lasts less than two weeks. Although it is not related to influenza, in the U.S. and U.K., it is sometimes called the "stomach flu".

Travelers' diarrhea (TD) is a stomach and intestinal infection. TD is defined as the passage of unformed stool while traveling. It may be accompanied by abdominal cramps, nausea, fever, headache and bloating. Occasionally bloody diarrhea may occur. Most travelers recover within three to four days with little or no treatment. About 12% of people may have symptoms for a week.
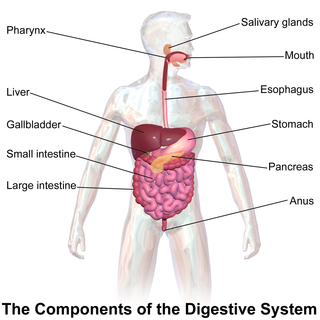
Gastrointestinal diseases refer to diseases involving the gastrointestinal tract, namely the esophagus, stomach, small intestine, large intestine and rectum; and the accessory organs of digestion, the liver, gallbladder, and pancreas.

Small intestinal bacterial overgrowth (SIBO), also termed bacterial overgrowth, or small bowel bacterial overgrowth syndrome (SBBOS), is a disorder of excessive bacterial growth in the small intestine. Unlike the colon, which is rich with bacteria, the small bowel usually has fewer than 100,000 organisms per millilitre. Patients with bacterial overgrowth typically develop symptoms which may include nausea, bloating, vomiting, diarrhea, malnutrition, weight loss, and malabsorption by various mechanisms.
Tropical sprue is a malabsorption disease commonly found in tropical regions, marked with abnormal flattening of the villi and inflammation of the lining of the small intestine. It differs significantly from coeliac sprue. It appears to be a more severe form of environmental enteropathy.

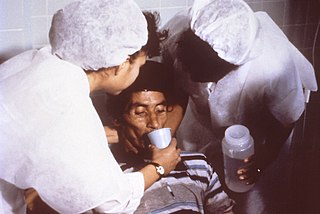
Oral rehydration therapy (ORT) is a type of fluid replacement used to prevent and treat dehydration, especially due to diarrhea. It involves drinking water with modest amounts of sugar and salts, specifically sodium and potassium. Oral rehydration therapy can also be given by a nasogastric tube. Therapy can include the use of zinc supplements to reduce the duration of diarrhea in infants and children under the age of 5. Use of oral rehydration therapy has been estimated to decrease the risk of death from diarrhea by up to 93%.

Colestyramine (INN) or cholestyramine (USAN) is a bile acid sequestrant, which binds bile in the gastrointestinal tract to prevent its reabsorption. It is a strong ion exchange resin, which means it can exchange its chloride anions with anionic bile acids in the gastrointestinal tract and bind them strongly in the resin matrix. The functional group of the anion exchange resin is a quaternary ammonium group attached to an inert styrene-divinylbenzene copolymer.
Enterotoxigenic Escherichia coli (ETEC) is a type of Escherichia coli and one of the leading bacterial causes of diarrhea in the developing world, as well as the most common cause of travelers' diarrhea. Insufficient data exists, but conservative estimates suggest that each year, about 157,000 deaths occur, mostly in children, from ETEC. A number of pathogenic isolates are termed ETEC, but the main hallmarks of this type of bacterium are expression of one or more enterotoxins and presence of fimbriae used for attachment to host intestinal cells. The bacterium was identified by the Bradley Sack lab in Kolkata in 1968.
Rifaximin, is a non-absorbable, broad spectrum antibiotic mainly used to treat travelers' diarrhea. It is based on the rifamycin antibiotics family. Since its approval in Italy in 1987, it has been licensed in over more than 30 countries for the treatment of a variety of gastrointestinal diseases like irritable bowel syndrome, and hepatic encephalopathy. It acts by inhibiting RNA synthesis in susceptible bacteria by binding to the RNA polymerase enzyme. This binding blocks translocation, which stops transcription. It is marketed under the brand name Xifaxan by Salix Pharmaceuticals.
Antibiotic-associated diarrhea (AAD) results from an imbalance in the colonic microbiota caused by antibiotics. Microbiotal alteration changes carbohydrate metabolism with decreased short-chain fatty acid absorption and an osmotic diarrhea as a result. Another consequence of antibiotic therapy leading to diarrhea is an overgrowth of potentially pathogenic organisms such as Clostridioides difficile. It is defined as frequent loose and watery stools with no other complications.
Chronic diarrheaof infancy, also called toddler's diarrhea, is a common condition typically affecting up to 1.7 billion children between ages 6–30 months worldwide every year, usually resolving by age 4. According to the World Health Organization (WHO), diarrheal disease is the second greatest cause of death in children 5 years and younger. Diarrheal disease takes the lives of 525,000 or more children per year. Diarrhea is characterized as the condition of passing of three or more loose or watery bowel movements within a day sometimes with undigested food visible. Diarrhea is separated into three clinical categories; acute diarrhea may last multiple hours or days, acute bloody diarrhea, also known as dysentery, and finally, chronic or persistent diarrhea which lasts 2–4 weeks or more. There is normal growth with no evidence of malnutrition in the child experiencing persistent diarrhea. In chronic diarrhea there is no evidence of blood in the stool and there is no sign of infection. The condition may be related to irritable bowel syndrome. There are various tests that can be performed to rule out other causes of diarrhea that don't fall under the chronic criteria, including blood test, colonoscopy, and even genetic testing. Most acute or severe cases of diarrhea have treatment guidelines revolving around prescription or non prescription medications based on the cause, but the treatment protocols for chronic diarrhea focus on replenishing the body with lost fluids and electrolytes, because there typically isn't a treatable cause.
Probiotics are live microorganisms promoted with claims that they provide health benefits when consumed, generally by improving or restoring the gut flora. Probiotics are considered generally safe to consume, but may cause bacteria-host interactions and unwanted side effects in rare cases. There is little evidence that probiotics bring the health benefits claimed for them.
Bile acid malabsorption (BAM), known also as bile acid diarrhea, is a cause of several gut-related problems, the main one being chronic diarrhea. It has also been called bile acid-induced diarrhea, cholerheic or choleretic enteropathy, bile salt diarrhea or bile salt malabsorption. It can result from malabsorption secondary to gastrointestinal disease, or be a primary disorder, associated with excessive bile acid production. Treatment with bile acid sequestrants is often effective. Depending on the severity of symptoms, it may be recognised as a disability in the United Kingdom under the Equality Act 2010.
Dehydration can occur as a result of diarrhea, vomiting, water scarcity, physical activity, and alcohol consumption. Management of dehydration seeks to reverse dehydration by replenishing the lost water and electrolytes. Water and electrolytes can be given through a number of routes, including oral, intravenous, and rectal.
Clostridioides difficile is a bacterium known for causing serious diarrheal infections, and may also cause colon cancer. It is known also as C. difficile, or C. diff, and is a Gram-positive species of spore-forming bacteria. Clostridioides spp. are anaerobic, motile bacteria, ubiquitous in nature and especially prevalent in soil. Its vegetative cells are rod-shaped, pleomorphic, and occur in pairs or short chains. Under the microscope, they appear as long, irregular cells with a bulge at their terminal ends. Under Gram staining, C. difficile cells are Gram-positive and show optimum growth on blood agar at human body temperatures in the absence of oxygen. C. difficile is catalase- and superoxide dismutase-negative, and produces up to three types of toxins: enterotoxin A, cytotoxin B and Clostridioides difficile transferase. Under stress conditions, the bacteria produce spores that are able to tolerate extreme conditions that the active bacteria cannot tolerate.






