
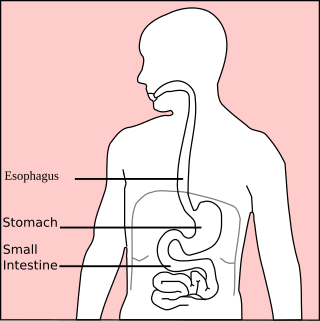
Peptic ulcer disease is a break in the inner lining of the stomach, the first part of the small intestine, or sometimes the lower esophagus. An ulcer in the stomach is called a gastric ulcer, while one in the first part of the intestines is a duodenal ulcer. The most common symptoms of a duodenal ulcer are waking at night with upper abdominal pain, and upper abdominal pain that improves with eating. With a gastric ulcer, the pain may worsen with eating. The pain is often described as a burning or dull ache. Other symptoms include belching, vomiting, weight loss, or poor appetite. About a third of older people with peptic ulcers have no symptoms. Complications may include bleeding, perforation, and blockage of the stomach. Bleeding occurs in as many as 15% of cases.

Helicobacter pylori, previously known as Campylobacter pylori, is a gram-negative, flagellated, helical bacterium. Mutants can have a rod or curved rod shape, that exhibit less virulence. Its helical body is thought to have evolved to penetrate the mucous lining of the stomach, helped by its flagella, and thereby establish infection. The bacterium was first identified as the causal agent of gastric ulcers in 1983 by the Australian doctors Barry Marshall and Robin Warren. In 2005 they were awarded the Nobel Prize in Physiology or Medicine for this discovery.

Stomach cancer, also known as gastric cancer, is a cancer that develops from the lining of the stomach. Most cases of stomach cancers are gastric carcinomas, which can be divided into a number of subtypes, including gastric adenocarcinomas. Lymphomas and mesenchymal tumors may also develop in the stomach. Early symptoms may include heartburn, upper abdominal pain, nausea, and loss of appetite. Later signs and symptoms may include weight loss, yellowing of the skin and whites of the eyes, vomiting, difficulty swallowing, and blood in the stool, among others. The cancer may spread from the stomach to other parts of the body, particularly the liver, lungs, bones, lining of the abdomen, and lymph nodes.

Delta cells are somatostatin-producing cells. They can be found in the stomach, intestine and the pancreatic islets. Delta cells comprise ca 5% of the cells in the islets but may interact with many more islet cells than suggested by their low numbers. In rodents, delta-cells are located in the periphery of the islets; in humans the islet architecture is generally less organized and delta-cells are frequently observed inside the islets as well. In both species, the peptide hormone Urocortin III (Ucn3) is a major local signal that is released from beta cells to induce the local secretion of somatostatin. It has also been suggested that somatostatin may be implicated in insulin-induced hypoglycaemia through a mechanism involving SGLT-2 receptors. Ghrelin can also strongly stimulate somatostatin secretion, thus indirectly inhibiting insulin release. Viewed under an electron microscope, delta-cells can be identified as cells with smaller and slightly more compact granules than beta cells.

Intrinsic factor (IF), cobalamin binding intrinsic factor, also known as gastric intrinsic factor (GIF), is a glycoprotein produced by the parietal cells (in humans) or chief cells (in rodents) of the stomach. It is necessary for the absorption of vitamin B12 later on in the distal ileum of the small intestine. In humans, the gastric intrinsic factor protein is encoded by the CBLIF gene. Haptocorrin (transcobalamin I) is another glycoprotein secreted by the salivary glands which binds to vitamin B12. Vitamin B12 is acid-sensitive and in binding to haptocorrin it can safely pass through the acidic stomach to the duodenum.

Pernicious anemia is a disease where not enough red blood cells are produced due to a deficiency of vitamin B12. Those affected often have a gradual onset. The most common initial symptoms are feeling tired and weak. Other symptoms may include shortness of breath, feeling faint, a smooth red tongue, pale skin, chest pain, nausea and vomiting, loss of appetite, heartburn, numbness in the hands and feet, difficulty walking, memory loss, muscle weakness, poor reflexes, blurred vision, clumsiness, depression, and confusion. Without treatment, some of these problems may become permanent.
Gastrin is a peptide hormone that stimulates secretion of gastric acid (HCl) by the parietal cells of the stomach and aids in gastric motility. It is released by G cells in the pyloric antrum of the stomach, duodenum, and the pancreas.

Parietal cells (also known as oxyntic cells) are epithelial cells in the stomach that secrete hydrochloric acid (HCl) and intrinsic factor. These cells are located in the gastric glands found in the lining of the fundus and body regions of the stomach. They contain an extensive secretory network of canaliculi from which the HCl is secreted by active transport into the stomach. The enzyme hydrogen potassium ATPase (H+/K+ ATPase) is unique to the parietal cells and transports the H+ against a concentration gradient of about 3 million to 1, which is the steepest ion gradient formed in the human body. Parietal cells are primarily regulated via histamine, acetylcholine and gastrin signalling from both central and local modulators.

A gastrectomy is a partial or total surgical removal of the stomach.

Gastritis is the inflammation of the lining of the stomach. It may occur as a short episode or may be of a long duration. There may be no symptoms but, when symptoms are present, the most common is upper abdominal pain. Other possible symptoms include nausea and vomiting, bloating, loss of appetite and heartburn. Complications may include stomach bleeding, stomach ulcers, and stomach tumors. When due to autoimmune problems, low red blood cells due to not enough vitamin B12 may occur, a condition known as pernicious anemia.

Achlorhydria and hypochlorhydria refer to states where the production of hydrochloric acid in gastric secretions of the stomach and other digestive organs is absent or low, respectively. It is associated with various other medical problems.
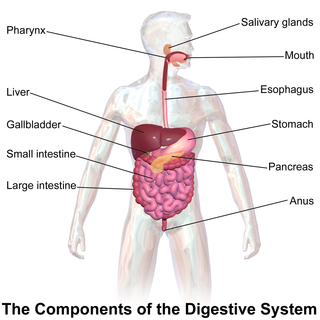
Gastrointestinal diseases refer to diseases involving the gastrointestinal tract, namely the esophagus, stomach, small intestine, large intestine and rectum; and the accessory organs of digestion, the liver, gallbladder, and pancreas.

MALT lymphoma is a form of lymphoma involving the mucosa-associated lymphoid tissue (MALT), frequently of the stomach, but virtually any mucosal site can be affected. It is a cancer originating from B cells in the marginal zone of the MALT.

Gastric antral vascular ectasia (GAVE) is an uncommon cause of chronic gastrointestinal bleeding or iron deficiency anemia. The condition is associated with dilated small blood vessels in the gastric antrum, which is a distal part of the stomach. The dilated vessels result in intestinal bleeding. It is also called watermelon stomach because streaky long red areas that are present in the stomach may resemble the markings on watermelon.

Gastric glands are glands in the lining of the stomach that play an essential role in the process of digestion. Their secretions make up the digestive gastric juice. The gastric glands open into gastric pits in the mucosa. The gastric mucosa is covered in surface mucous cells that produce the mucus necessary to protect the stomach's epithelial lining from gastric acid secreted by parietal cells in the glands, and from pepsin, a secreted digestive enzyme. Surface mucous cells follow the indentations and partly line the gastric pits. Other mucus secreting cells are found in the necks of the glands. These are mucous neck cells that produce a different kind of mucus.

Ménétrier disease is a rare, acquired, premalignant disease of the stomach characterized by massive gastric folds, excessive mucus production with resultant protein loss, and little or no acid production (achlorhydria). The disorder is associated with excessive secretion of transforming growth factor alpha (TGF-α). It is named after a French physician Pierre Eugène Ménétrier, 1859–1935.
This is a timeline of the events relating to the discovery that peptic ulcer disease and some cancers are caused by H. pylori. In 2005, Barry Marshall and Robin Warren were awarded the Nobel Prize in Physiology or Medicine for their discovery that peptic ulcer disease (PUD) was primarily caused by Helicobacter pylori, a bacterium with affinity for acidic environments, such as the stomach. As a result, PUD that is associated with H. pylori is currently treated with antibiotics used to eradicate the infection. For decades prior to their discovery, it was widely believed that PUD was caused by excess acid in the stomach. During this time, acid control was the primary method of treatment for PUD, to only partial success. Among other effects, it is now known that acid suppression alters the stomach milieu to make it less amenable to H. pylori infection.

The gastric mucosa is the mucous membrane layer of the stomach, which contains the gastric pits, to which the gastric glands empty. In humans, it is about one mm thick, and its surface is smooth, soft, and velvety. It consists of simple secretory columnar epithelium, an underlying supportive layer of loose connective tissue called the lamina propria, and the muscularis mucosae, a thin layer of muscle that separates the mucosa from the underlying submucosa.
Stomach diseases include gastritis, gastroparesis, Crohn's disease and various cancers.
The gastric folds are coiled sections of tissue that exist in the mucosal and submucosal layers of the stomach. They provide elasticity by allowing the stomach to expand when a bolus enters it. These folds stretch outward through the action of mechanoreceptors, which respond to the increase in pressure. This allows the stomach to expand, therefore increasing the volume of the stomach without increasing pressure. They also provide the stomach with an increased surface area for nutrient absorption during digestion. Gastric folds may be seen during esophagogastroduodenoscopy or in radiological studies.



