Vaccine that either treats existing cancer or prevents development of cancer
This article is about therapeutic cancer vaccines. For preventive cancer vaccine, see Cancer immunoprevention.
A cancer vaccine, or oncovaccine, is a vaccine that either treats existing cancer or prevents development of cancer.[1] Vaccines that treat existing cancer are known as therapeutic cancer vaccines or tumor antigen vaccines. Some of the vaccines are "autologous", being prepared from samples taken from the patient, and are specific to that patient.
Some researchers claim that cancerous cells routinely arise and are destroyed by the immune system (immunosurveillance);[2] and that tumors form when the immune system fails to destroy them.[3]
One approach to cancer vaccination is to separate proteins from cancer cells and immunize patients against those proteins as antigens, in the hope of stimulating the immune system to kill the cancer cells. Research on cancer vaccines is underway for treatment of breast, lung, colon, skin, kidney, prostate and other cancers.[6]
Another approach is to generate an immune response in situ in the patient using oncolytic viruses. This approach was used in the drug talimogene laherparepvec, a variant of herpes simplex virus engineered to selectively replicate in tumor tissue and to express the immune stimulatory protein GM-CSF. This enhances the anti-tumor immune response to tumor antigens released following viral lysis and provides a patient-specific vaccine.[7]
Mechanism of action
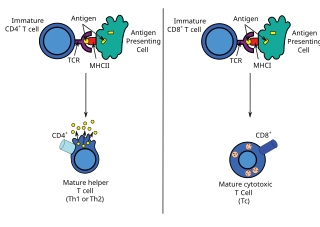
Tumor antigen vaccines work the same way that viral vaccines work, by training the immune system to attack cells that contain the antigens in the vaccine. The difference is that the antigens for viral vaccines are derived from viruses or cells infected with virus, while the antigens for tumor antigen vaccines are derived from cancer cells. Since tumor antigens are antigens found in cancer cells but not normal cells, vaccinations containing tumor antigens should train the immune system to target cancer cells not healthy cells. Cancer-specific tumor antigens include peptides from proteins that are not typically found in normal cells but are activated in cancer cells or peptides containing cancer-specific mutations. Antigen-presenting cells (APCs) such as dendritic cells take up antigens from the vaccine, process them into epitopes, and present the epitopes to T-cells via Major Histocompatibility Complex proteins. If T-cells recognize the epitope as foreign, the adaptive immune system is activated and target cells that express the antigens.[8]
Prevention vs. treatment
Viral vaccines usually work by preventing the spread of the virus. Similarly, cancer vaccines can be designed to target common antigens before cancer evolves if an individual has appropriate risk factors. Additional preventive applications include preventing the cancer from evolving further or undergoing metastasis and preventing relapse after remission. Therapeutic vaccines focus on killing existing tumors. While cancer vaccines have generally been demonstrated to be safe, their efficacy still needs improvement. One way to potentially improve vaccine therapy is by combining the vaccine with other types of immunotherapy aimed at stimulating the immune system. Since tumors often evolve mechanisms to suppress the immune system, immune checkpoint blockade has recently received a lot of attention as a potential treatment to be combined with vaccines. For therapeutic vaccines, combined therapies can be more aggressive, but greater care to ensure the safety of relatively healthy patients is needed for combinations involving preventive vaccines.[9]
Types
Cancer vaccines can be cell-based, protein- or peptide-based, gene-based (DNA/RNA).[9] or using live attenuated bacterial or viral organisms.[10]
Cell-based vaccines include tumor cells or tumor cell lysates. Tumor cells from the patient are predicted to contain the greatest spectrum of relevant antigens, but this approach is expensive and often requires too many tumor cells from the patient to be effective.[11] Using a combination of established cancer cell lines that resemble the patient's tumor can overcome these barriers, but this approach has yet to be effective. Canvaxin, which incorporates three melanoma cell lines, failed phase III clinical trials.[11] Another cell-based vaccine strategy involves autologous dendritic cells (dendritic cells derived from the patient) to which tumor antigens are added. In this strategy, the antigen-presenting dendritic cells directly stimulate T-cells rather than relying on processing of the antigens by native APCs after the vaccine is delivered. The best known dendritic cell vaccine is Sipuleucel-T (Provenge), which only improved survival by four months. The efficacy of dendritic cell vaccines may be limited due to difficulty in getting the cells to migrate to lymph nodes and interact with T-cells.[9]
Peptide-based vaccines usually consist of cancer specific-epitopes and often require an adjuvant (for example, GM-CSF) to stimulate the immune system and enhance antigenicity.[8] Examples of these epitopes include Her2 peptides, such as GP2 and NeuVax. However, this approach requires MHC profiling of the patient because of MHC restriction.[12] The need for MHC profile selection can be overcome by using longer peptides ("synthetic long peptides") or purified protein, which are then processed into epitopes by APCs.[12]
Gene-based vaccines are composed of the nucleic acid (DNA/RNA) encoding for the gene. The gene is then expressed in APCs and the resulting protein product is processed into epitopes. Delivery of the gene is particularly challenging for this type of vaccine.[9] At least one drug candidate, mRNA-4157/V940, is investigating newly developed mRNA vaccines for use in this application.[13][14]
On April 14, 2009, Dendreon Corporation announced that their Phase III clinical trial of sipuleucel-T, a cancer vaccine designed to treat prostate cancer, had demonstrated an increase in survival. It received U.S. Food and Drug Administration (FDA) approval for use in the treatment of advanced prostate cancer patients on April 29, 2010.[16][17]
Interim results from a phase III trial of talimogene laherparepvec in melanoma showed a significant tumour response compared to administration of GM-CSF alone.[7]
A recent Trial Watch review (2015) of peptide-based vaccines summarized the results of more than 60 trials that were published in the 13 months preceding the article.[12] These trials targeted hematological malignancies (cancers of the blood), melanoma (skin cancer), breast cancer, head and neck cancer, gastroesophageal cancer, lung cancer, pancreatic cancer, prostate cancer, ovarian cancer, and colorectal cancers. The antigens included peptides from HER2, telomerase (TERT), survivin (BIRC5), and Wilms' tumor 1 (WT1). Several trials also used "personalized" mixtures of 12-15 distinct peptides. That is, they contain a mixture of peptides from the patient's tumor that the patient exhibits an immune response against. The results of these studies indicate that these peptide vaccines have minimal side effects and suggest that they induce targeted immune responses in patients treated with the vaccines. The article also discusses 19 clinical trials that were initiated in the same time period. These trials are targeting solid tumors, glioma, glioblastoma, melanoma, and breast, cervical, ovarian, colorectal, and non-small lung cell cancers and include antigens from MUC1, IDO1 (Indoleamine 2,3-dioxygenase), CTAG1B, and two VEGF receptors, FLT1 and KDR. Notably, the IDO1 vaccine is being tested in patients with melanoma in combination with the immune checkpoint inhibitor ipilimumab and the BRAF (gene) inhibitor vemurafenib.
The following table, summarizing information from another recent review shows an example of the antigen used in the vaccine tested in Phase 1/2 clinical trials for each of 10 different cancers:[11]
CimaVax-EGF was approved in Cuba in 2011.[19] Similar to Oncophage, it is not yet approved for use in the United States, although it is already undergoing phase II trials to that end.[20][21]
Bacillus Calmette-Guérin (BCG) was approved by the FDA in 1990 as a vaccine for early-stage bladder cancer.[22] BCG can be administered intravesically (directly into the bladder) or as an adjuvant in other cancer vaccines.
Abandoned research
CancerVax (Canvaxin), Genitope Corp (MyVax personalized immunotherapy), and FavId FavId (Favrille Inc) are examples of cancer vaccine projects that have been terminated, due to poor phase III and IV results.[citation needed]
Desirable characteristics
Cancer vaccines seek to target a tumor-specific antigen as distinct from self-proteins. Selection of the appropriate adjuvant to activate antigen-presenting cells to stimulate immune responses, is required. Bacillus Calmette-Guérin, an aluminum-based salt, and a squalene-oil-water emulsion are approved for clinical use. An effective vaccine should also stimulate long term immune memory to prevent tumor recurrence. Some scientists claim both the innate and adaptive immune systems must be activated to achieve total tumor elimination.[23]
Antigen candidates
Tumor antigens have been divided into two categories: shared tumor antigens; and unique tumor antigens. Shared antigens are expressed by many tumors. Unique tumor antigens result from mutations induced through physical or chemical carcinogens; they are therefore expressed only by individual tumors.
In one approach, vaccines contain whole tumor cells, though these vaccines have been less effective in eliciting immune responses in spontaneous cancer models. Defined tumor antigens decrease the risk of autoimmunity, but because the immune response is directed to a single epitope, tumors can evade destruction through antigen loss variance. A process called "epitope spreading" or "provoked immunity" may mitigate this weakness, as sometimes an immune response to a single antigen can lead to immunity against other antigens on the same tumor.[23]
For example, since Hsp70 plays an important role in the presentation of antigens of destroyed cells including cancer cells,[24] this protein may be used as an effective adjuvant in the development of antitumor vaccines.[25]
Hypothesized problems
A vaccine against a particular virus is relatively easy to create. The virus is foreign to the body, and therefore expresses antigens that the immune system can recognize. Furthermore, viruses usually only provide a few viable variants. By contrast, developing vaccines for viruses that mutate constantly such as influenza or HIV has been problematic. A tumor can have many cell types of cells, each with different cell-surface antigens. Those cells are derived from each patient and display few if any antigens that are foreign to that individual. This makes it difficult for the immune system to distinguish cancer cells from normal cells. Some scientists believe that renal cancer and melanoma are the two cancers with most evidence of spontaneous and effective immune responses, possibly because they often display antigens that are evaluated as foreign. Many attempts at developing cancer vaccines are directed against these tumors. However, Provenge's success in prostate cancer, a disease that never spontaneously regresses, suggests that cancers other than melanoma and renal cancer may be equally amenable to immune attack.[citation needed]
However, most vaccine clinical trials have failed or had modest results according to the standard RECIST criteria.[26] The precise reasons are unknown, but possible explanations include:
Disease stage too advanced: bulky tumor deposits actively suppress the immune system using mechanisms such as secretion of cytokines that inhibit immune activity. The most suitable stage for a cancer vaccine is likely to be early, when the tumor volume is low, which complicates the trial process, which take upwards of five years and require many patients to reach measurable end points. One alternative is to target patients with residual disease after surgery, radiotherapy or chemotherapy that does not harm the immune system.
Escape loss variants (that target a single tumor antigen) are likely to be less effective. Tumors are heterogeneous and antigen expression differs markedly between tumors (even in the same patient). The most effective vaccine is likely to raise an immune response against a broad range of tumor antigens to minimise the chance of the tumor mutating and becoming resistant to the therapy.
Prior treatments may have modified tumors in ways that nullify the vaccine. (Numerous clinical trials treated patients following chemotherapy that may destroy the immune system. Patients who are immune suppressed are not good candidates for vaccines.)
Some tumors progress rapidly and/or unpredictably, and they can outpace the immune system. Developing a mature immune response to a vaccine may require months, but some cancers (e.g. advanced pancreatic) can kill patients in less time.
Many cancer vaccine clinical trials target patients' immune responses. Correlations typically show that the patients with the strongest immune responses lived the longest, offering evidence that the vaccine is working. An alternative explanation is that patients with the best immune responses were healthier patients with a better prognosis, and would have survived longest even without the vaccine.
Recommendations
In January 2009, a review article made recommendations for successful oncovaccine development as follows:[27]
Target settings with a low disease burden.
Conduct randomized Phase II trials so that the Phase III program is sufficiently powered.
Do not randomize antigen plus adjuvant versus adjuvant alone. The goal is to establish clinical benefit of the immunotherapy (i.e., adjuvanted vaccine) over the standard of care. The adjuvant may have a low-level clinical effect that skews the trial, increasing the chances of a false negative.
Base development decisions on clinical data rather than immune responses. Time-to-event end points are more valuable and clinically relevant.
Design regulatory into the program from inception; invest in manufacturing and product assays early.
In immunology, an antigen (Ag) is a molecule, moiety, foreign particulate matter, or an allergen, such as pollen, that can bind to a specific antibody or T-cell receptor. The presence of antigens in the body may trigger an immune response.
Immunotherapy or biological therapy is the treatment of disease by activating or suppressing the immune system. Immunotherapies designed to elicit or amplify an immune response are classified as activation immunotherapies, while immunotherapies that reduce or suppress are classified as suppression immunotherapies. Immunotherapy is under preliminary research for its potential to treat various forms of cancer.
Cancer immunotherapy (immuno-oncotherapy) is the stimulation of the immune system to treat cancer, improving the immune system's natural ability to fight the disease. It is an application of the fundamental research of cancer immunology (immuno-oncology) and a growing subspecialty of oncology.
An antigen-presenting cell (APC) or accessory cell is a cell that displays an antigen bound by major histocompatibility complex (MHC) proteins on its surface; this process is known as antigen presentation. T cells may recognize these complexes using their T cell receptors (TCRs). APCs process antigens and present them to T cells.
Ipilimumab, sold under the brand name Yervoy, is a monoclonal antibody medication that works to activate the immune system by targeting CTLA-4, a protein receptor that downregulates the immune system.
Vaccine therapy is a type of treatment that uses a substance or group of substances to stimulate the immune system to destroy a tumor or infectious microorganisms such as bacteria or viruses.
Adoptive cell transfer (ACT) is the transfer of cells into a patient. The cells may have originated from the patient or from another individual. The cells are most commonly derived from the immune system with the goal of improving immune functionality and characteristics. In autologous cancer immunotherapy, T cells are extracted from the patient, genetically modified and cultured in vitro and returned to the same patient. Comparatively, allogeneic therapies involve cells isolated and expanded from a donor separate from the patient receiving the cells.
Dendreon Pharmaceuticals LLC is a biotechnology company. Its lead product, Provenge, is an immunotherapy for prostate cancer. It consists of a mixture of the patient's own blood cells that have been incubated with the Dendreon PAP-GM-CSF fusion protein. Phase III clinical trial results demonstrating a survival benefit for prostate cancer patients receiving the drug were presented at the AUA meeting on April 28, 2009. After going through the approval process, Provenge was given full approval by the FDA on April 29, 2010. Dendreon's stock value fell 66% on August 4, 2011, after abandoning its forecast for its debut drug Provenge.
Peptide-based synthetic vaccines are subunit vaccines made from peptides. The peptides mimic the epitopes of the antigen that triggers direct or potent immune responses. Peptide vaccines can not only induce protection against infectious pathogens and non-infectious diseases but also be utilized as therapeutic cancer vaccines, where peptides from tumor-associated antigens are used to induce an effective anti-tumor T-cell response.
Neuvenge, Lapuleucel-T, is a therapeutic cancer vaccine (TCV) in development by Dendreon (DNDN). It uses the "immunotherapy platform approach" first successfully demonstrated on the U.S. Food and Drug Administration (FDA)-approved TCV Provenge. It was first tested on breast cancer patients with tumors expressing HER2/neu, and is now scheduled to be tested on bladder cancer patients.
Gustav Gaudernack is a scientist working in the development of cancer vaccines and cancer immunotherapy. He has developed various strategies in immunological treatment of cancer. He is involved in several ongoing cellular and immuno-gene therapeutic clinical trials and his research group has put major efforts into the development of various T cell-based immunotherapeutic strategies.
ALECSAT technology is a novel method of epigenetic cancer immunotherapy being used by the company CytoVac. It uses a patient's own immune system to target tumor cells in prostate cancer, glioblastomas, and potentially pancreatic cancer. ALECSAT research, directed by Alexei Kirken and Karine Dzhandzhugazyan, has led to several clinical trials.
Eftilagimod alpha is a large-molecule cancer drug being developed by the clinical-stage biotechnology company Immutep. Efti is a soluble version of the immune checkpoint molecule LAG-3. It is an APC Activator used to increase an immune response to tumors, and is administered by subcutaneous injection. Efti has three intended clinical settings:
Cancer/testis (CT) antigens are a group of proteins united by their importance in development and in cancer immunotherapy. In general, expression of these proteins is restricted to male germ cells in the adult animal. However, in cancer these developmental antigens are often re-expressed and can serve as a locus of immune activation. Thus, they are often classified as tumor antigens. The expression of CT antigens in various malignancies is heterogeneous and often correlates with tumor progression. CT antigens have been described in melanoma, liver cancer, lung cancer, bladder cancer, and pediatric tumors such as neuroblastoma. Gametogenesis offers an important role for many of these antigens in the differentiation, migration, and cell division of primordial germ cells, spermatogonia spermatocytes and spermatids. Because of their tumor-restricted expression and strong in vivo immunogenicity, CT antigens are identified as ideal targets for tumor specific immunotherapeutic approaches and prompted the development of several clinical trials of CT antigens-based vaccine therapy. CT antigens have been found to have at least 70 families so far, including about 140 members, most of which are expressed during spermatogenesis. Their expression are mainly regulated by epigenetic events, specifically, DNA methylation.
T lymphocytes are cells of the immune system that attack and destroy virus-infected cells, tumor cells and cells from transplanted organs. This occurs because each T cell is endowed with a highly specific receptor that can bind to an antigen present at the surface of another cell. The T cell receptor binds to a complex formed by a surface protein named "MHC" and a small peptide of about 9 amino-acids, which is located in a groove of the MHC molecule. This peptide can originate from a protein that remains within the cell. Whereas each T cell recognizes a single antigen, collectively the T cells are endowed with a large diversity of receptors targeted at a wide variety of antigens. T cells originate in the thymus. There a process named central tolerance eliminates the T cells that have a receptor recognizing an antigen present on normal cells of the organism. This enables the T cells to eliminate cells with "foreign" or "abnormal" antigens without harming the normal cells.
The dendritic cell-based cancer vaccine is an innovation in therapeutic strategy for cancer patients.
Cancer vaccine targeting CD4+ T cells is a type of vaccine used to treat existing cancer. Cancerous cells usually cannot be recognized by the human immune system, and therefore cannot be destroyed. Some researchers state that cancer can be treated by increasing the response of T cells, especially CD4+ T cells, to cancerous cells through cancer vaccine injection.
Neoepitopes are a class of major histocompatibility complex (MHC) bounded peptides. They represent the antigenic determinants of neoantigens. Neoepitopes are recognized by the immune system as targets for T cells and can elicit immune response to cancer.
Individualized cancer immunotherapy, also referred to as individualized immuno-oncology, is a novel concept for therapeutic cancer vaccines that are truly personalized to a single individual.
A therapeutic vaccine is a vaccine which is administered after a disease or infection has already occurred. A therapeutic vaccine works by activating the immune system of a patient to fight an infection. A therapeutic vaccine differs from a prophylactic vaccine in that prophylactic vaccines are administered to individuals as a precautionary measure to avoid the infection or disease while therapeutic vaccines are administered after the individual is already affected by the disease or infection. A therapeutic vaccine fights an existing infection in the body rather than immunizing the body for protection against future diseases and infections. Therapeutic vaccines are mostly used against viral infections. Patients affected with chronic viral infections are administered with therapeutic vaccines, as their immune system is not able to produce enough efficient antibodies.
↑ Babu RA, Kumar KK, Reddy GS, Anuradha C (2010). "Cancer Vaccine: A Review". Journal of Orofacial Sciences. 2 (3): 77–82. doi:10.4103/0975-8844.103507 (inactive 1 November 2024). S2CID68256825.{{cite journal}}: CS1 maint: DOI inactive as of November 2024 (link)
↑ Giarelli E (October 2007). "Cancer vaccines: a new frontier in prevention and treatment". Oncology. 21 (11 Suppl Nurse Ed): 11–7, discussion 18. PMID18154203.
1 2 Amgen press release. Amgen announces top-line results of phase 3 talimogene laherparepvec trial in melanoma. Mar 19, 2013. Available hereArchived 21 January 2014 at the Wayback Machine
↑ Nishikawa M, Takemoto S, Takakura Y (April 2008). "Heat shock protein derivatives for delivery of antigens to antigen presenting cells". International Journal of Pharmaceutics. Special Issue in Honor of Prof. Tsuneji Nagai. 354 (1–2): 23–27. doi:10.1016/j.ijpharm.2007.09.030. PMID17980980.
↑ Savvateeva LV, Schwartz AM, Gorshkova LB, Gorokhovets NV, Makarov VA, Reddy VP, etal. (1 January 2015). "Prophylactic Admission of an In Vitro Reconstructed Complexes of Human Recombinant Heat Shock Proteins and Melanoma Antigenic Peptides Activates Anti-Melanoma Responses in Mice". Current Molecular Medicine. 15 (5): 462–468. doi:10.2174/1566524015666150630125024. PMID26122656.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.