
A carbohydrate is an biomolecule consisting of carbon (C), hydrogen (H) and oxygen (O) atoms, usually with a hydrogen–oxygen atom ratio of 2:1 and thus with the empirical formula Cm(H2O)n, which does not mean the H has covalent bonds with O. However, not all carbohydrates conform to this precise stoichiometric definition, nor are all chemicals that do conform to this definition automatically classified as carbohydrates.
Dieting is the practice of eating food in a regulated way to decrease, maintain, or increase body weight, or to prevent and treat diseases such as diabetes and obesity. As weight loss depends on calorie intake, different kinds of calorie-reduced diets, such as those emphasising particular macronutrients, have been shown to be no more effective than one another. As weight regain is common, diet success is best predicted by long-term adherence. Regardless, the outcome of a diet can vary widely depending on the individual.
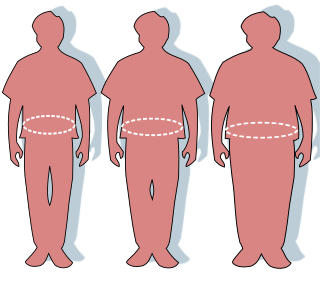
Obesity is a medical condition, sometimes considered a disease, in which excess body fat has accumulated to such an extent that it can potentially have negative effects on health. People are classified as obese when their body mass index (BMI)—a person's weight divided by the square of the person's height—is over 30 kg/m2; the range 25–30 kg/m2 is defined as overweight. Some East Asian countries use lower values to calculate obesity. Obesity is a major cause of disability and is correlated with various diseases and conditions, particularly cardiovascular diseases, type 2 diabetes, obstructive sleep apnea, certain types of cancer, and osteoarthritis.

Weight loss, in the context of medicine, health, or physical fitness, refers to a reduction of the total body mass, by a mean loss of fluid, body fat, or lean mass. Weight loss can either occur unintentionally because of malnourishment or an underlying disease, or from a conscious effort to improve an actual or perceived overweight or obese state. "Unexplained" weight loss that is not caused by reduction in calorific intake or increase in exercise is called cachexia and may be a symptom of a serious medical condition.

Low-carbohydrate diets restrict carbohydrate consumption relative to the average diet. Foods high in carbohydrates are limited, and replaced with foods containing a higher percentage of fat and protein, as well as low carbohydrate foods.
Basal metabolic rate (BMR) is the rate of energy expenditure per unit time by endothermic animals at rest. It is reported in energy units per unit time ranging from watt (joule/second) to ml O2/min or joule per hour per kg body mass J/(h·kg). Proper measurement requires a strict set of criteria to be met. These criteria include being in a physically and psychologically undisturbed state and being in a thermally neutral environment while in the post-absorptive state (i.e., not actively digesting food). In bradymetabolic animals, such as fish and reptiles, the equivalent term standard metabolic rate (SMR) applies. It follows the same criteria as BMR, but requires the documentation of the temperature at which the metabolic rate was measured. This makes BMR a variant of standard metabolic rate measurement that excludes the temperature data, a practice that has led to problems in defining "standard" rates of metabolism for many mammals.

Weight gain is an increase in body weight. This can involve an increase in muscle mass, fat deposits, excess fluids such as water or other factors. Weight gain can be a symptom of a serious medical condition.
Calorie restriction is a dietary regimen that reduces the energy intake from foods and beverages without incurring malnutrition. The possible effect of calorie restriction on body weight management, longevity, and aging-associated diseases has been an active area of research.

A high-protein diet is a diet in which 20% or more of the total daily calories come from protein. Many high protein diets are high in saturated fat and restrict intake of carbohydrates.

A healthy diet is a diet that maintains or improves overall health. A healthy diet provides the body with essential nutrition: fluid, macronutrients such as protein, micronutrients such as vitamins, and adequate fibre and food energy.
Specific dynamic action (SDA), also known as thermic effect of food (TEF) or dietary induced thermogenesis (DIT), is the amount of energy expenditure above the basal metabolic rate due to the cost of processing food for use and storage. Heat production by brown adipose tissue which is activated after consumption of a meal is an additional component of dietary induced thermogenesis. The thermic effect of food is one of the components of metabolism along with resting metabolic rate and the exercise component. A commonly used estimate of the thermic effect of food is about 10% of one's caloric intake, though the effect varies substantially for different food components. For example, dietary fat is very easy to process and has very little thermic effect, while protein is hard to process and has a much larger thermic effect.

A very-low-calorie diet (VLCD), also known as semistarvation diet and crash diet, is a type of diet with very or extremely low daily food energy consumption. VLCDs are defined as a diet of 800 kilocalories (3,300 kJ) per day or less. Modern medically supervised VLCDs use total meal replacements, with regulated formulations in Europe and Canada which contain the recommended daily requirements for vitamins, minerals, trace elements, fatty acids, protein and electrolyte balance. Carbohydrates may be entirely absent, or substituted for a portion of the protein; this choice has important metabolic effects. Medically supervised VLCDs have specific therapeutic applications for rapid weight loss, such as in morbid obesity or before a bariatric surgery, using formulated, nutritionally complete liquid meals containing 800 kilocalories or less per day for a maximum of 12 weeks.
A diabetic diet is a diet that is used by people with diabetes mellitus or high blood sugar to minimize symptoms and dangerous complications of long-term elevations in blood sugar.
A low-fat diet is one that restricts fat, and often saturated fat and cholesterol as well. Low-fat diets are intended to reduce the occurrence of conditions such as heart disease and obesity. For weight loss, they perform similarly to a low-carbohydrate diet, since macronutrient composition does not determine weight loss success. Fat provides nine calories per gram while carbohydrates and protein each provide four calories per gram. The Institute of Medicine recommends limiting fat intake to 35% of total calories to control saturated fat intake.

The Western pattern diet is a modern dietary pattern that is generally characterized by high intakes of pre-packaged foods, refined grains, red meat, processed meat, high-sugar drinks, candy and sweets, fried foods, industrially produced animal products, butter and other high-fat dairy products, eggs, potatoes, corn, and low intakes of fruits, vegetables, whole grains, pasture-raised animal products, fish, nuts, and seeds.
Intermittent fasting is any of various meal timing schedules that cycle between voluntary fasting and non-fasting over a given period. Methods of intermittent fasting include alternate-day fasting, periodic fasting, such as the 5:2 diet, and daily time-restricted eating.

Diet plays an important role in the genesis of obesity. Personal choices, food advertising, social customs and cultural influences, as well as food availability and pricing all play a role in determining what and how much an individual eats.
Hedonic hunger or hedonic hyperphagia is the "drive to eat to obtain pleasure in the absence of an energy deficit". Particular foods may have a high "hedonic rating" or individuals may have increased susceptibility to environmental food cues. Weight loss programs may aim to control or to compensate for hedonic hunger. Therapeutic interventions may influence hedonic eating behavior.
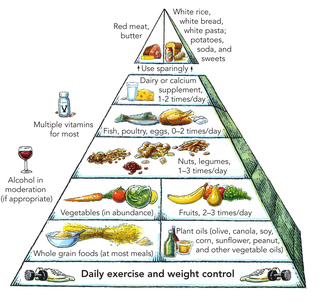
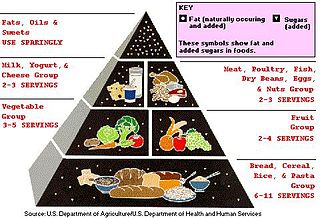
Preventive Nutrition is a branch of nutrition science with the goal of preventing, delaying, and/or reducing the impacts of disease and disease-related complications. It is concerned with a high level of personal well-being, disease prevention, and diagnosis of recurring health problems or symptoms of discomfort which are often precursors to health issues. The overweight and obese population numbers have increased over the last 40 years and numerous chronic diseases are associated with obesity. Preventive nutrition may assist in prolonging the onset of non-communicable diseases and may allow adults to experience more "healthy living years." There are various ways of educating the public about preventive nutrition. Information regarding preventive nutrition is often communicated through public health forums, government programs and policies, or nutritional education. For example, in the United States, preventive nutrition is taught to the public through the use of the food pyramid or MyPlate initiatives.
The Summermatter cycle is a physiological concept describing the complex relationship between physical activity/inactivity and energy expenditure/conservation.











