
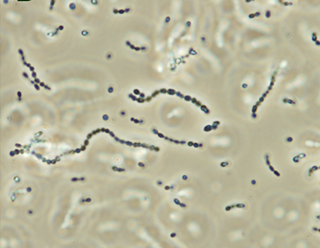
Streptococcus is a genus of gram-positive coccus or spherical bacteria that belongs to the family Streptococcaceae, within the order Lactobacillales, in the phylum Bacillota. Cell division in streptococci occurs along a single axis, so as they grow, they tend to form pairs or chains that may appear bent or twisted. This differs from staphylococci, which divide along multiple axes, thereby generating irregular, grape-like clusters of cells. Most streptococci are oxidase-negative and catalase-negative, and many are facultative anaerobes.

Erysipelas is a relatively common bacterial infection of the superficial layer of the skin, extending to the superficial lymphatic vessels within the skin, characterized by a raised, well-defined, tender, bright red rash, typically on the face or legs, but which can occur anywhere on the skin. It is a form of cellulitis and is potentially serious.

Group A streptococcal infections are a number of infections with Streptococcus pyogenes, a group A streptococcus (GAS). S. pyogenes is a species of beta-hemolytic Gram-positive bacteria that is responsible for a wide range of infections that are mostly common and fairly mild. If the bacteria enter the bloodstream an infection can become severe and life-threatening, and is called an invasive GAS (iGAS).

Streptococcus pyogenes is a species of Gram-positive, aerotolerant bacteria in the genus Streptococcus. These bacteria are extracellular, and made up of non-motile and non-sporing cocci that tend to link in chains. They are clinically important for humans, as they are an infrequent, but usually pathogenic, part of the skin microbiota that can cause Group A streptococcal infection. S. pyogenes is the predominant species harboring the Lancefield group A antigen, and is often called group A Streptococcus (GAS). However, both Streptococcus dysgalactiae and the Streptococcus anginosus group can possess group A antigen as well. Group A streptococci, when grown on blood agar, typically produce small (2–3 mm) zones of beta-hemolysis, a complete destruction of red blood cells. The name group A (beta-hemolytic) Streptococcus is thus also used.

Scarlet fever, also known as scarlatina, is an infectious disease caused by Streptococcus pyogenes, a Group A streptococcus (GAS). It most commonly affects children between five and 15 years of age. The signs and symptoms include a sore throat, fever, headache, swollen lymph nodes, and a characteristic rash. The face is flushed and the rash is red and blanching. It typically feels like sandpaper and the tongue may be red and bumpy. The rash occurs as a result of capillary damage by exotoxins produced by S.pyogenes. On darker-pigmented skin the rash may be hard to discern.

Streptococcal pharyngitis, also known as streptococcal sore throat, is pharyngitis caused by Streptococcus pyogenes, a gram-positive, group A streptococcus. Common symptoms include fever, sore throat, red tonsils, and enlarged lymph nodes in the front of the neck. A headache and nausea or vomiting may also occur. Some develop a sandpaper-like rash which is known as scarlet fever. Symptoms typically begin one to three days after exposure and last seven to ten days.

Pharyngitis is inflammation of the back of the throat, known as the pharynx. It typically results in a sore throat and fever. Other symptoms may include a runny nose, cough, headache, difficulty swallowing, swollen lymph nodes, and a hoarse voice. Symptoms usually last 3–5 days, but can be longer depending on cause. Complications can include sinusitis and acute otitis media. Pharyngitis is a type of upper respiratory tract infection.

Necrotizing fasciitis (NF), also known as flesh-eating disease, is a bacterial infection that results in the death of parts of the body's soft tissue. It is a severe disease of sudden onset that spreads rapidly. Symptoms usually include red or purple skin in the affected area, severe pain, fever, and vomiting. The most commonly affected areas are the limbs and perineum.

Cellulitis is usually a bacterial infection involving the inner layers of the skin. It specifically affects the dermis and subcutaneous fat. Signs and symptoms include an area of redness which increases in size over a few days. The borders of the area of redness are generally not sharp and the skin may be swollen. While the redness often turns white when pressure is applied, this is not always the case. The area of infection is usually painful. Lymphatic vessels may occasionally be involved, and the person may have a fever and feel tired.
Tonsillitis is inflammation of the tonsils in the upper part of the throat. It can be acute or chronic. Acute tonsillitis typically has a rapid onset. Symptoms may include sore throat, fever, enlargement of the tonsils, trouble swallowing, and enlarged lymph nodes around the neck. Complications include peritonsillar abscess (Quinsy).

Group B streptococcal infection, also known as Group B streptococcal disease or just Group B strep infection, is the infectious disease caused by the bacterium Streptococcus agalactiae, which is the most common human pathogen belonging to the group B of the Lancefield classification of streptococci—hence the group B stretococcal (GBS) infection nomenclature. Infection with GBS can cause serious illness and sometimes death, especially in newborns, the elderly, and people with compromised immune systems. The most severe form of group B streptococcal disease is neonatal meningitis in infants, which is frequently lethal and can cause permanent neuro-cognitive impairment.

Lymphangitis is an inflammation or an infection of the lymphatic channels that occurs as a result of infection at a site distal to the channel. It may present as long red streaks spreading away from the site of infection. It is a possible medical emergency as involvement of the lymphatic system allows for an infection to spread rapidly. The most common cause of lymphangitis in humans is bacteria, in which case sepsis and death could result within hours if left untreated. The most commonly involved bacteria include Streptococcus pyogenes and hemolytic streptococci. In some cases, it can be caused by viruses such as mononucleosis or cytomegalovirus, as well as specific conditions such as tuberculosis or syphilis, and the fungus Sporothrix schenckii. Lymphangitis is sometimes mistakenly called "blood poisoning". In reality, "blood poisoning" is synonymous with sepsis.
A skin infection is an infection of the skin in humans and other animals, that can also affect the associated soft tissues such as loose connective tissue and mucous membranes. They comprise a category of infections termed skin and skin structure infections (SSSIs), or skin and soft tissue infections (SSTIs), and acute bacterial SSSIs (ABSSSIs). They are distinguished from dermatitis, although skin infections can result in skin inflammation.

Orbital cellulitis is inflammation of eye tissues behind the orbital septum. It is most commonly caused by an acute spread of infection into the eye socket from either the adjacent sinuses or through the blood. It may also occur after trauma. When it affects the rear of the eye, it is known as retro-orbital cellulitis.

Arcanobacterium haemolyticum is a species of bacteria classified as a gram-positive bacillus. It is catalase-negative, facultative anaerobic, beta-hemolytic, and not motile. It has been known to cause head and neck infections, pharyngitis, and sinusitis.

Streptococcus canis is a group G beta-hemolytic species of Streptococcus. It was first isolated in dogs, giving the bacterium its name. These bacteria are characteristically different from Streptococcus dysgalactiae, which is a human-specific group G species that has a different phenotypic chemical composition. S. canis is important to the skin and mucosal health of cats and dogs, but under certain circumstances, these bacteria can cause opportunistic infections. These infections were known to afflict dogs and cats prior to the formal description of the species in Devriese et al., 1986. However, additional studies revealed cases of infection in other mammal species, including cattle and even humans. Instances of mortality from S. canis in humans are very low with only a few reported cases, while actual instances of infection may be underreported due to mischaracterizations of the bacteria as S. dysgalactiae. This species, in general, is highly susceptible to antibiotics, and plans to develop a vaccine to prevent human infections are currently being considered.

Streptococcus dysgalactiae is a gram positive, beta-haemolytic, coccal bacterium belonging to the family Streptococcaceae. It is capable of infecting both humans and animals, but is most frequently encountered as a commensal of the alimentary tract, genital tract, or less commonly, as a part of the skin flora. The clinical manifestations in human disease range from superficial skin-infections and tonsillitis, to severe necrotising fasciitis and bacteraemia. The incidence of invasive disease has been reported to be rising. Several different animal species are susceptible to infection by S. dysgalactiae, but bovine mastitis and infectious arthritis in lambs have been most frequently reported.
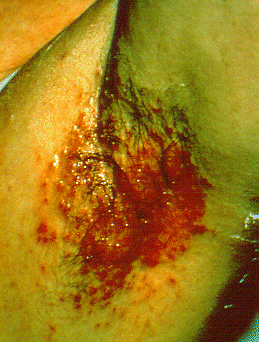
Streptococcal intertrigo is a skin condition that is secondary to a streptococcal bacterial infection. It is often seen in infants and young children and can be characterized by a fiery-red color of the skin, foul odor with an absence of satellite lesions, and skin softening in the neck, armpits or folds of the groin. Newborn children and infants commonly develop intertrigo because of physical features such as deep skin folds, short neck, and flexed posture. Prompt diagnosis by a medical professional and treatment with topical and/or oral antibiotics can effectively relieve symptoms.
Streptococcus iniae is a species of Gram-positive, sphere-shaped bacterium belonging to the genus Streptococcus. Since its isolation from an Amazon freshwater dolphin in the 1970s, S. iniae has emerged as a leading fish pathogen in aquaculture operations worldwide, resulting in over US$100M in annual losses. Since its discovery, S. iniae infections have been reported in at least 27 species of cultured or wild fish from around the world. Freshwater and saltwater fish including tilapia, red drum, hybrid striped bass, and rainbow trout are among those susceptible to infection by S. iniae. Infections in fish manifest as meningoencephalitis, skin lesions, and septicemia.
Streptococcosis is an infectious disease caused by bacteria of the genus Steptococcus. This disease is most common among horses, guinea pigs, dogs, cats, and fish with symptoms varying based on the streptococcal species involved. In humans, this disease typically involves a throat infection and is called streptococcal pharyngitis or strep throat.


