
Hearing loss is a partial or total inability to hear. Hearing loss may be present at birth or acquired at any time afterwards. Hearing loss may occur in one or both ears. In children, hearing problems can affect the ability to acquire spoken language, and in adults it can create difficulties with social interaction and at work. Hearing loss can be temporary or permanent. Hearing loss related to age usually affects both ears and is due to cochlear hair cell loss. In some people, particularly older people, hearing loss can result in loneliness. Deaf people usually have little to no hearing.
Tinnitus is a variety of sound that is heard when no corresponding external sound is present. Nearly everyone experiences faint "normal tinnitus" in a completely quiet room; but it is of concern only if it is bothersome, interferes with normal hearing, or is associated with other problems. The word tinnitus comes from the Latin tinnire, "to ring". In some people, it interferes with concentration, and can be associated with anxiety and depression.

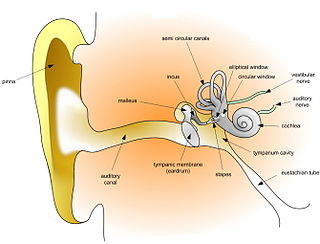
The cochlea is the part of the inner ear involved in hearing. It is a spiral-shaped cavity in the bony labyrinth, in humans making 2.75 turns around its axis, the modiolus. A core component of the cochlea is the organ of Corti, the sensory organ of hearing, which is distributed along the partition separating the fluid chambers in the coiled tapered tube of the cochlea.

The vestibulocochlear nerve or auditory vestibular nerve, also known as the eighth cranial nerve, cranial nerve VIII, or simply CN VIII, is a cranial nerve that transmits sound and equilibrium (balance) information from the inner ear to the brain. Through olivocochlear fibers, it also transmits motor and modulatory information from the superior olivary complex in the brainstem to the cochlea.
Ototoxicity is the property of being toxic to the ear (oto-), specifically the cochlea or auditory nerve and sometimes the vestibular system, for example, as a side effect of a drug. The effects of ototoxicity can be reversible and temporary, or irreversible and permanent. It has been recognized since the 19th century. There are many well-known ototoxic drugs used in clinical situations, and they are prescribed, despite the risk of hearing disorders, for very serious health conditions. Ototoxic drugs include antibiotics, loop diuretics, and platinum-based chemotherapy agents. A number of nonsteroidal anti-inflammatory drugs (NSAIDS) have also been shown to be ototoxic. This can result in sensorineural hearing loss, dysequilibrium, or both. Some environmental and occupational chemicals have also been shown to affect the auditory system and interact with noise.

The acoustic reflex is an involuntary muscle contraction that occurs in the middle ear in response to loud sound stimuli or when the person starts to vocalize.
Sensorineural hearing loss (SNHL) is a type of hearing loss in which the root cause lies in the inner ear or sensory organ or the vestibulocochlear nerve. SNHL accounts for about 90% of reported hearing loss. SNHL is usually permanent and can be mild, moderate, severe, profound, or total. Various other descriptors can be used depending on the shape of the audiogram, such as high frequency, low frequency, U-shaped, notched, peaked, or flat.

Audiometry is a branch of audiology and the science of measuring hearing acuity for variations in sound intensity and pitch and for tonal purity, involving thresholds and differing frequencies. Typically, audiometric tests determine a subject's hearing levels with the help of an audiometer, but may also measure ability to discriminate between different sound intensities, recognize pitch, or distinguish speech from background noise. Acoustic reflex and otoacoustic emissions may also be measured. Results of audiometric tests are used to diagnose hearing loss or diseases of the ear, and often make use of an audiogram.
Auditory neuropathy (AN) is a hearing disorder in which the outer hair cells of the cochlea are present and functional, but sound information is not transmitted sufficiently by the auditory nerve to the brain. Hearing loss with AN can range from normal hearing sensitivity to profound hearing loss.
Presbycusis, or age-related hearing loss, is the cumulative effect of aging on hearing. It is a progressive and irreversible bilateral symmetrical age-related sensorineural hearing loss resulting from degeneration of the cochlea or associated structures of the inner ear or auditory nerves. The hearing loss is most marked at higher frequencies. Hearing loss that accumulates with age but is caused by factors other than normal aging is not presbycusis, although differentiating the individual effects of distinct causes of hearing loss can be difficult.

An audiogram is a graph that shows the audible threshold for standardized frequencies as measured by an audiometer. The Y axis represents intensity measured in decibels (dB) and the X axis represents frequency measured in hertz (Hz). The threshold of hearing is plotted relative to a standardised curve that represents 'normal' hearing, in dB(HL). They are not the same as equal-loudness contours, which are a set of curves representing equal loudness at different levels, as well as at the threshold of hearing, in absolute terms measured in dB SPL.
The auditory brainstem response (ABR), also called brainstem evoked response audiometry (BERA), is an auditory evoked potential extracted from ongoing electrical activity in the brain and recorded via electrodes placed on the scalp. The measured recording is a series of six to seven vertex positive waves of which I through V are evaluated. These waves, labeled with Roman numerals in Jewett and Williston convention, occur in the first 10 milliseconds after onset of an auditory stimulus. The ABR is considered an exogenous response because it is dependent upon external factors.
Noise-induced hearing loss (NIHL) is a hearing impairment resulting from exposure to loud sound. People may have a loss of perception of a narrow range of frequencies or impaired perception of sound including sensitivity to sound or ringing in the ears. When exposure to hazards such as noise occur at work and is associated with hearing loss, it is referred to as occupational hearing loss.
Pure-tone audiometry is the main hearing test used to identify hearing threshold levels of an individual, enabling determination of the degree, type and configuration of a hearing loss and thus providing a basis for diagnosis and management. Pure-tone audiometry is a subjective, behavioural measurement of a hearing threshold, as it relies on patient responses to pure tone stimuli. Therefore, pure-tone audiometry is only used on adults and children old enough to cooperate with the test procedure. As with most clinical tests, standardized calibration of the test environment, the equipment and the stimuli is needed before testing proceeds. Pure-tone audiometry only measures audibility thresholds, rather than other aspects of hearing such as sound localization and speech recognition. However, there are benefits to using pure-tone audiometry over other forms of hearing test, such as click auditory brainstem response (ABR). Pure-tone audiometry provides ear specific thresholds, and uses frequency specific pure tones to give place specific responses, so that the configuration of a hearing loss can be identified. As pure-tone audiometry uses both air and bone conduction audiometry, the type of loss can also be identified via the air-bone gap. Although pure-tone audiometry has many clinical benefits, it is not perfect at identifying all losses, such as ‘dead regions’ of the cochlea and neuropathies such as auditory processing disorder (APD). This raises the question of whether or not audiograms accurately predict someone's perceived degree of disability.

Hearing, or auditory perception, is the ability to perceive sounds through an organ, such as an ear, by detecting vibrations as periodic changes in the pressure of a surrounding medium. The academic field concerned with hearing is auditory science.
Auditory fatigue is defined as a temporary loss of hearing after exposure to sound. This results in a temporary shift of the auditory threshold known as a temporary threshold shift (TTS). The damage can become permanent if sufficient recovery time is not allowed before continued sound exposure. When the hearing loss is rooted from a traumatic occurrence, it may be classified as noise-induced hearing loss, or NIHL.
Acoustic trauma is the sustainment of an injury to the eardrum as a result of a very loud noise. Its scope usually covers loud noises with a short duration, such as an explosion, gunshot or a burst of loud shouting. Quieter sounds that are concentrated in a narrow frequency may also cause damage to specific frequency receptors. The range of severity can vary from pain to hearing loss.
An audiologist, according to the American Academy of Audiology, "is a person who, by virtue of academic degree, clinical training, and license to practice and/or professional credential, is uniquely qualified to provide a comprehensive array of professional services related to the prevention of hearing loss and the audiologic identification, assessment, diagnosis, and treatment of persons with impairment of auditory and vestibular function, and to the prevention of impairments associated with them."
Identification of a hearing loss is usually conducted by a general practitioner medical doctor, otolaryngologist, certified and licensed audiologist, school or industrial audiometrist, or other audiometric technician. Diagnosis of the cause of a hearing loss is carried out by a specialist physician or otorhinolaryngologist.
Computational audiology is a branch of audiology that employs techniques from mathematics and computer science to improve clinical treatments and scientific understanding of the auditory system. Computational audiology is closely related to computational medicine, which uses quantitative models to develop improved methods for general disease diagnosis and treatment.





