
Mastectomy is the medical term for the surgical removal of one or both breasts, partially or completely. A mastectomy is usually carried out to treat breast cancer. In some cases, women believed to be at high risk of breast cancer have the operation as a preventive measure. Alternatively, some women can choose to have a wide local excision, also known as a lumpectomy, an operation in which a small volume of breast tissue containing the tumor and a surrounding margin of healthy tissue is removed to conserve the breast. Both mastectomy and lumpectomy are referred to as "local therapies" for breast cancer, targeting the area of the tumor, as opposed to systemic therapies, such as chemotherapy, hormonal therapy, or immunotherapy.

Breast cancer is a cancer that develops from breast tissue. Signs of breast cancer may include a lump in the breast, a change in breast shape, dimpling of the skin, milk rejection, fluid coming from the nipple, a newly inverted nipple, or a red or scaly patch of skin. In those with distant spread of the disease, there may be bone pain, swollen lymph nodes, shortness of breath, or yellow skin.

Paget's disease of the breast is a rare skin change at the nipple nearly always associated with underlying breast cancer. Paget's disease of the breast was first described by Sir James Paget in 1874. The condition is an uncommon disease accounting for 1 to 4% of all breast cancers cases. 92% to 100% of patients with Paget's disease of the breast have an underlying breast cancer.
Inflammatory breast cancer (IBC) is one of the most aggressive types of breast cancer. It can occur in women of any age. It is referred to as "inflammatory" due to its frequent presentation with symptoms resembling a skin inflammation, such as erysipelas.

Lumpectomy is a surgical removal of a discrete portion or "lump" of breast tissue, usually in the treatment of a malignant tumor or breast cancer. It is considered a viable breast conservation therapy, as the amount of tissue removed is limited compared to a full-breast mastectomy, and thus may have physical and emotional advantages over more disfiguring treatment. Sometimes a lumpectomy may be used to either confirm or rule out that cancer has actually been detected. A lumpectomy is usually recommended to patients whose cancer has been detected early and who do not have enlarged tumors. Although a lumpectomy is used to allow for most of the breast to remain intact, the procedure may result in adverse affects that can include sensitivity and result in scar tissue, pain, and possible disfiguration of the breast if the lump taken out is significant. According to National Comprehensive Cancer Network guidelines, lumpectomy may be performed for ductal carcinoma in situ (DCIS), invasive ductal carcinoma, or other conditions.

Invasive carcinoma of no special type, invasive breast carcinoma of no special type (IBC-NST), invasive ductal carcinoma (IDC), infiltrating ductal carcinoma (IDC) or invasive ductal carcinoma, not otherwise specified (NOS) is a disease. For international audiences this article will use "invasive carcinoma NST" because it is the preferred term of the World Health Organization (WHO).

Microcalcifications are tiny deposits of calcium salts that are too small to be felt but can be detected by imaging.
Breast cancer management takes different approaches depending on physical and biological characteristics of the disease, as well as the age, over-all health and personal preferences of the patient. Treatment types can be classified into local therapy and systemic treatment. Local therapy is most efficacious in early stage breast cancer, while systemic therapy is generally justified in advanced and metastatic disease, or in diseases with specific phenotypes.

Breast cancer screening is the medical screening of asymptomatic, apparently healthy women for breast cancer in an attempt to achieve an earlier diagnosis. The assumption is that early detection will improve outcomes. A number of screening tests have been employed, including clinical and self breast exams, mammography, genetic screening, ultrasound, and magnetic resonance imaging.
Breast-conserving surgery refers to an operation that aims to remove breast cancer while avoiding a mastectomy. Different forms of this operation include: lumpectomy (tylectomy), wide local excision, segmental resection, and quadrantectomy. Breast-conserving surgery has been increasingly accepted as an alternative to mastectomy in specific patients, as it provides tumor removal while maintaining an acceptable cosmetic outcome. This page reviews the history of this operation, important considerations in decision making and patient selection, and the emerging field of oncoplastic breast conservation surgery.
Comedocarcinoma is a kind of breast cancer that demonstrates comedonecrosis, which is the central necrosis of cancer cells within involved ducts. Comedocarcinomas are usually non-infiltrating and intraductal tumors, characterized as a comedo-type, high-grade ductal carcinoma in situ (DCIS). However, there have been accounts of comedocarcinoma which has then diversified into other cell types and developed into infiltrating (invasive) ductal carcinoma. Recurrence and survival rates differ for invasive breast cancer which has originated as comedocarcinoma compared with other types of cancer cells.

Lobular carcinoma in situ (LCIS) is an incidental microscopic finding with characteristic cellular morphology and multifocal tissue patterns. The condition is a laboratory diagnosis and refers to unusual cells in the lobules of the breast. The lobules and acini of the terminal duct-lobular unit (TDLU), the basic functional unit of the breast, may become distorted and undergo expansion due to the abnormal proliferation of cells comprising the structure. These changes represent a spectrum of atypical epithelial lesions that are broadly referred to as lobular neoplasia (LN).

Male breast cancer (MBC) is a cancer in males that originates in their breasts. Males account for less than 1% of new breast cancers with about 20,000 new cases being diagnosed worldwide every year. Its incidence rates in males vs. females are, respectively, 0.4 and 66.7 per 100,000 person-years. The worldwide incidences of male as well as female breast cancers have been increasing over the last few decades. Currently, one of every 800 men are estimated to develop this cancer during their lifetimes.
The term nonpuerperal mastitis describes inflammatory lesions of the breast (mastitis) that occur unrelated to pregnancy and breastfeeding.

Atypical ductal hyperplasia (ADH) is the term used for a benign lesion of the breast that indicates an increased risk of breast cancer.

A breast biopsy is usually done after a suspicious lesion is discovered on either mammography or ultrasound to get tissue for pathological diagnosis. Several methods for a breast biopsy now exist. The most appropriate method of biopsy for a patient depends upon a variety of factors, including the size, location, appearance and characteristics of the abnormality. The different types of breast biopsies include fine-needle aspiration (FNA), vacuum-assisted biopsy, core needle biopsy, and surgical excision biopsy. Breast biopsies can be done utilizing ultrasound, MRI or a stereotactic biopsy imaging guidance. Vacuum assisted biopsies are typically done using stereotactic techniques when the suspicious lesion can only be seen on mammography. On average, 5–10 biopsies of a suspicious breast lesion will lead to the diagnosis of one case of breast cancer. Needle biopsies have largely replaced open surgical biopsies in the initial assessment of imaging as well as palpable abnormalities in the breast.
Dynamic angiothermography (DATG) is a technique for the diagnosis of breast cancer. This technique, though springing from the previous conception of thermography, is based on a completely different principle. DATG records the temperature variations linked to the vascular changes in the breast due to angiogenesis. The presence, change, and growth of tumors and lesions in breast tissue change the vascular network in the breast. Consequently, through measuring the vascular structure over time, DATG effectively monitors the change in breast tissue due to tumors and lesions. It is currently used in combination with other techniques for diagnosis of breast cancer. This diagnostic method is a low-cost one compared with other techniques.
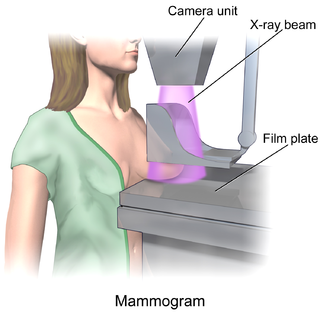
In medicine, breast imaging is a sub-speciality of diagnostic radiology that involves imaging of the breasts for screening or diagnostic purposes. There are various methods of breast imaging using a variety of technologies as described in detail below. Traditional screening and diagnostic mammography uses x-ray technology and has been the mainstay of breast imaging for many decades. Breast tomosynthesis is a relatively new digital x-ray mammography technique that produces multiple image slices of the breast similar to, but distinct from, computed tomography (CT). Xeromammography and galactography are somewhat outdated technologies that also use x-ray technology and are now used infrequently in the detection of breast cancer. Breast ultrasound is another technology employed in diagnosis and screening that can help differentiate between fluid filled and solid lesions, an important factor to determine if a lesion may be cancerous. Breast MRI is a technology typically reserved for high-risk patients and patients recently diagnosed with breast cancer. Lastly, scintimammography is used in a subgroup of patients who have abnormal mammograms or whose screening is not reliable on the basis of using traditional mammography or ultrasound.
Papillary carcinomas of the breast (PCB), also termed malignant papillary carcinomas of the breast, are rare forms of the breast cancers. The World Health Organization (2019) classified papillary neoplasms of the breast into 5 types: intraductal papilloma, papillary ductal carcinoma in situ (PDCIS), encapsulated papillary carcinoma (EPC), solid-papillary carcinoma (SPC), and invasive papillary carcinoma (IPC). The latter four carcinomas are considered here; intraductal papilloma is a benign neoplasm. The World Health Organization regarded solid papillary carcinoma as having two subtypes: in situ and invasive SPC.

Pure apocrine carcinoma of the breast (PACB) is a rare carcinoma derived from the epithelial cells in the lactiferous ducts of the mammary gland. The mammary gland is an apocrine gland. Its lactiferous ducts have two layers of epithelial cells, a luminal layer which faces the duct's lumen and a basal layer which lies beneath the luminal layer. There are at least four subtypes of epithelial cells in these ducts: luminal progenitor cells and luminal mature cells which reside in the luminal layer and mammary stem cells and basal cells which reside in the basal layer. Examination of the genes expressed in PACB cancer cells indicate that most of these tumors consist of cells derived from luminal cells but a minority of these tumors consist of cells derived from basal cells.











