
A football player or footballer is a sportsperson who plays one of the different types of football. The main types of football are association football, American football, Canadian football, Australian rules football, Gaelic football, rugby league, and rugby union.

Sports injuries are injuries that occur during sports, or exercising in general. In the United States, there are approximately 30 million people who participate in some form of organized sports. Of those 30 million, about 3 million athletes aged 14 and under suffered a sports injury annually. According to a study performed at Stanford University, 21% of the injuries observed in elite college athletes caused them to miss at least one day of sports activity, and approximately 77% of these injuries involved the knee, leg, ankle, or foot. The leading death-causing sports injury is traumatic head or neck injuries.

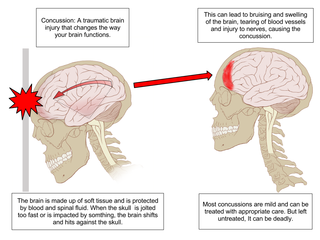
A concussion, also known as a mild traumatic brain injury (mTBI), is a head injury that temporarily affects brain functioning. Symptoms may include loss of consciousness; memory loss; headaches; difficulty with thinking, concentration, or balance; nausea; blurred vision; dizziness; sleep disturbances, and mood changes. Any of these symptoms may begin immediately, or appear days after the injury. Concussion should be suspected if a person indirectly or directly hits their head and experiences any of the symptoms of concussion. Symptoms of a concussion may be delayed by 1–2 days after the accident. It is not unusual for symptoms to last 2 weeks in adults and 4 weeks in children. Fewer than 10% of sports-related concussions among children are associated with loss of consciousness.

Health issues in American football comprise a large number of health risks associated with participating in the sport. Injuries are relatively common in American football, due to its nature as a full-contact game. Injuries occur during both practice and games. Several factors can affect the frequency of injuries: epidemiological studies have shown older players can be at a greater risk, while equipment and experienced coaches can reduce the risk of injury. Common injuries include strains, sprains, fractures, dislocations, and concussions. Concussions have become a concern, as they increase the risk of mental illnesses like dementia and chronic traumatic encephalopathy (CTE). In individual leagues like the National Football League (NFL) and National Collegiate Athletic Association (NCAA), a public injury report is published containing all injured players on a team, their injury and the game-day status of each player.

Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease linked to repeated trauma to the head. The encephalopathy symptoms can include behavioral problems, mood problems, and problems with thinking. The disease often gets worse over time and can result in dementia.
Second-impact syndrome (SIS) occurs when the brain swells rapidly, and catastrophically, after a person has a second concussion before symptoms from an earlier one have subsided. This second blow may occur minutes, days, or weeks after an initial concussion, and even the mildest grade of concussion can lead to second impact syndrome. The condition is often fatal, and almost everyone who is not killed is severely disabled. The cause of SIS is uncertain, but it is thought that the brain's arterioles lose their ability to regulate their diameter, and therefore lose control over cerebral blood flow, causing massive cerebral edema.
Concussion grading systems are sets of criteria used in sports medicine to determine the severity, or grade, of a concussion, the mildest form of traumatic brain injury. At least 16 such systems exist, and there is little agreement among professionals about which is the best to use. Several of the systems use loss of consciousness and amnesia as the primary determinants of the severity of the concussion.
The fencing response is an unnatural position of the arms following a concussion. Immediately after moderate forces have been applied to the brainstem, the forearms are held flexed or extended for a period lasting up to several seconds after the impact. The fencing response is often observed during athletic competition involving contact, such as combat sports, American football, ice hockey, rugby union, rugby league and Australian rules football. It is used as an overt indicator of injury force magnitude and midbrain localization to aid in injury identification and classification for events including on-field and/or bystander observations of sports-related head injuries.

The health issues of youth sports are concerns regarding the health and wellbeing of young people between the ages of 6 and 18 who participate in an organized sport. Given that these athletes are physically and mentally underdeveloped, they are particularly susceptible to heat illness, eating disorders and injury; sufficiently severe conditions can result in death. Awareness and prevention are key factors in preventing many health issues in youth sports.
Helmet-to-helmet collisions are occurrences in gridiron football when two players' football helmets make head-to-head contact with a high degree of force. Intentionally causing a helmet-to-helmet collision is a penalty in most football leagues, including many high school leagues.

Prevention of mild traumatic brain injury involves taking general measures to prevent traumatic brain injury, such as wearing seat belts, using airbags in cars, securing heavy furnitures and objects before earthquake or covering and holding under the table during an earthquake. Older people are encouraged to try to prevent falls, for example by keeping floors free of clutter and wearing thin, flat, shoes with hard soles that do not interfere with balance.
Concussions and play-related head blows in American football have been shown to be the cause of chronic traumatic encephalopathy (CTE), which has led to player deaths and other debilitating symptoms after retirement, including memory loss, depression, anxiety, headaches, stress, and sleep disturbances.

Schutt Sports was a United States company that manufactured protective gear for several sports, focusing on American football, baseball, softball, and lacrosse. Products manufactured by company, headquartered in Litchfield, Illinois, included helmets and other protections such as jockstraps, and shoulder pads. The company also produced American football sportswear including jerseys and pants.
A sports-related traumatic brain injury is a serious accident which may lead to significant morbidity or mortality. Traumatic brain injury (TBI) in sports are usually a result of physical contact with another person or stationary object, These sports may include boxing, gridiron football, field/ice hockey, lacrosse, martial arts, rugby, soccer, wrestling, auto racing, cycling, equestrian, rollerblading, skateboarding, skiing or snowboarding.
A traumatic brain injury (TBI) is a blow, jolt or penetration to the head that disrupts the function of the brain. Most TBIs are caused by falls, jumps, motor vehicle traffic crashes, being struck by a person or a blunt object, and assault. Student-athletes may be put at risk in school sports, creating concern about concussions and brain injury. A concussion can be caused by a direct blow to the head, or an indirect blow to the body that causes reactions in the brain. The result of a concussion is neurological impairment that may resolve spontaneously but may also have long-term consequences.
Head injuries in sports of any level are the most dangerous kind of injuries that can occur in sport, and are becoming more common in Australian sport. Concussions are the most common side effect of a head injury and are defined as "temporary unconsciousness or confusion and other symptoms caused by a blow to the head." A concussion also falls under the category of Traumatic Brain Injury (TBI). Especially in contact sports like Australian rules football and rugby, issues with concussions are prevalent, and methods to deal with, prevent and treat concussions are continuously being updated and researched to deal with the issue. Concussions pose a serious threat to the patients’ mental and physical health, as well as their playing career, and can result in lasting brain damage especially if left untreated. The signs that a player may have a concussion are: loss of consciousness or non-responsiveness, balance problems, a dazed, blank or vacant look and/or confusion and unawareness of their surroundings. Of course the signs are relevant only after the player experiences a blow to the head.
Concussions in professional rugby union are the most common injury received. Concussion can occur where an individual experiences an impact to the head, and are also notable in high-contact sports, including American football, boxing, MMA and Hockey. Concussions can occur in recreational activities like horse riding, jumping, cycling, and skiing as a result of forceful rotational moment, resulting in injuries to the brain due to the contact with the skull, giving the skull not enough time to move with the body, causing the brain to press against the skull. With the development of equipment and training methods, further education on identifying concussion symptoms, as well as adjustments to the terms of contact may allow players to make more informed decisions on their conduct on the pitch.
Most documented cases of chronic traumatic encephalopathy have occurred in many athletes involved in contact sports such as boxing, American football, wrestling, ice hockey, mixed martial arts, rugby and soccer. Other risk factors include being in the military, prior domestic violence, and repeated banging of the head. The exact amount of trauma required for the condition to occur is unknown. Below is a list of notable cases of CTE in sports.
A pediatric concussion, also known as pediatric mild traumatic brain injury (mTBI), is a head trauma that impacts the brain capacity. Concussion can affect functional, emotional, cognitive and physical factors and can occur in people of all ages. Symptoms following after the concussion vary and may include confusion, disorientation, lightheadedness, nausea, vomiting, blurred vision, loss of consciousness (LOC) and environment sensitivity. Concussion symptoms may vary based on the type, severity and location of the head injury. Concussion symptoms in infants, children, and adolescents often appear immediately after the injury, however, some symptoms may arise multiple days following the injury leading to a concussion. The majority of pediatric patients recover from the symptoms within one month following the injury. 10-30% of children and adolescents have a higher risk of a delayed recovery or of experiencing concussion symptoms that are persisting.
Michael J. Stuart is an American sports physician and orthopedic surgeon. He is a professor and vice-chairman of orthopedic surgery at the Mayo Clinic, and a co-director of the Mayo Clinic Sports Medicine Center. He has published more than 370 journal articles and 50 book chapters, as of 2022. He specializes in sports medicine, and advocates for strength, flexibility, and awareness, to reduce injuries in ice hockey. He collaborated to arrange the 2010, 2013 and 2017 Ice Hockey Summits, which focused on concussions, and educational programs for players, coaches and parents. His concussion research includes studying biomarkers, neuroimaging, and cognitive neuroscience. He argues that concussions are diagnosed more accurately with electroencephalography and the King-Devick Test eye test, and advocates their usage in sport.