Infections induced by C. perfringens are associated with tissue necrosis, bacteremia, emphysematous cholecystitis, and gas gangrene, which is also known as clostridial myonecrosis.[6] The specific name, perfringens, is derived from the Latinper (meaning "through") and frango ("burst"), referring to the disruption of tissue that occurs during gas gangrene.[7] Gas gangrene is caused by alpha toxin, or α-toxin, that embeds itself into the plasma membrane of cells and disrupts normal cellular function by altering membrane structure.[8] Research suggests that C. perfringens is capable of engaging in polymicrobial anaerobic infections.[9] It is commonly encountered in infections as a component of the normal flora. In this case, its role in disease is minor.[10]
C. perfringens toxins are a result of horizontal gene transfer of a neighboring cell's plasmids.[11] Shifts in genomic make-up are common for this species of bacterium and contribute to novel pathogenesis.[12] Major toxins are expressed differently in certain populations of C. perfringens; these populations are organized into strains based on their expressed toxins.[13] This especially impacts the food industry, as controlling this microbe is important for preventing foodborne illness.[12] Novel findings in C. perfringens hyper-motility, which was provisionally thought as non-motile, have been discovered as well.[14] Findings in metabolic processes reveal more information concerning C. perfringens pathogenic nature.[15]
Genome
Clostridium perfringens has a stable G+C content around 27 to 28 percent and average genome size of 3.5 Mb.[16] Genomes of 56 C. perfringens strains have since been made available on the NCBI genomes database for the scientific research community. Genomic research has revealed surprisingly high diversity in C. perfringenspangenome, with only 12.6 percent core genes, identified as the most divergent Gram-positive bacteria reported.[16] Nevertheless, 16S rRNA regions in between C. perfringens strains are found to be highly conserved (sequence identity >99.1%).[16]
The Clostridium perfringens enterotoxin (CPE)–producing strain has been identified to be a small portion of the overall C. perfringens population (~1-5%) through genomic testing.[17] Advances in genetic information surrounding strain A CPE C. perfringens has allowed techniques such as microbial source tracking (MST) to identify food contamination sources.[17] The CPE gene has been found within chromosomal DNA as well as plasmid DNA. Plasmid DNA has been shown to play and integral role in cell pathogenesis and encodes for major toxins, including CPE.[11]
C. perfringens has been shown to carry plasmid-containing genes for antibiotic resistance. The pCW3 plasmid is the primary conjugation plasmid responsible for creating antibiotic resistance in C. perfringens. Furthermore, the pCW3 plasmid also encodes for multiple toxins found in pathogenic strains of C. perfringens.[18] Antibiotic resistance genes observed thus far include tetracycline resistance, efflux protein, and aminoglycoside resistance.[19]
Within industrial contexts, such as food production, sequencing genomes for pathogenic strains of C. perfringens has become an expanding field of research. Poultry production is impacted directly from this trend as antibiotic-resistant strains of C. perfringens are becoming more common.[12] By performing a meta-genome analysis, researches are capable to identify novel strains of pathogenic bacterium, such as C. perfringens B20.[12]
Motility
Clostridium perfringens is provisionally identified as non-motile. They lack flagella; however, recent research suggests gliding as a form of motility.[20][21]
Hyper-motile variations
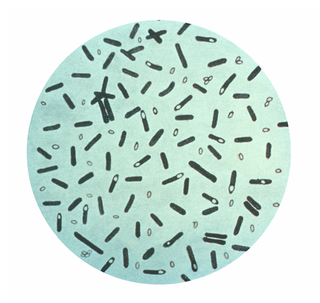
This illustration depicts a three-dimensional (3D), computer-generated image of a cluster of barrel-shaped, Clostridium perfringens bacteria. The artistic recreation was based upon scanning electron microscopic (SEM) imagery.
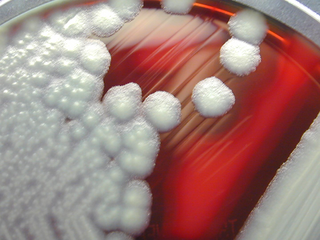
In agar plate cultures bacteria with hypermotile variations like SM101 frequently appear around the borders of the colonies. They create long thin filaments that enable them to move quickly, much like bacteria with flagella, according to video imaging of their gliding motion. The causes of the hypermotile phenotype and its immediate descendants were found using genome sequencing. The hypermotile offspring of strains SM101 and SM102, SM124 and SM127, respectively, had 10 and 6 nucleotide polymorphisms (SNPs) in comparison to their parent strains. The hypermotile strains have the common trait of gene mutations related to cell division.[20]
Regulation of gliding motility: The CpAL/VirSR system
Some strains of C. perfringens cause various diseases like gas gangrene and myonecrosis. Toxins produced that are required for myonecrosis is regulated by the C. perfringens Agr-like (CpAl) system through the VirSR two-component system. The CpAL/VirSR system is a quorum sensing system encoded by other pathogenic clostridia. Myonecrosis starts at the infection site and involves bacteria migrating deeper via gliding motility. Researchers investigated if the CpAL/VirSR system regulates gliding motility. The study demonstrated that the CpAL/VirSR regulates C. perfringens gliding motility. Additionally, the study suggests that gliding bacteria in myonecrosis have increased transcription of toxin genes.[21]
There are two methods of genetic manipulation via experimentation that have been shown to cause genetic transformation in C. perfringens.
Protoplast transformation
The first report of transformation in C. perfringens involved polyethyleneglycol-mediated transformation of protoplasts. The transformation procedure involved the addition of the plasmid DNA to the protoplasts in the presence of high concentrations of polyethylene glycol. During the first protoplast transformation experiment, L-phase variants of C. perfringens were generated by penicillin treatment in the presence 0.4m sucrose. After the transformation procedure was completed, all of the transformed cells were still in the form of L-phase variants. Reversion to vegetative cells was not obtained, but it was observed that autoplasts (protoplasts derived from autolysis) were able to be regenerated to produce rods with cell walls and could be transformed with C. perfringens plasmid DNA.[22]
Electroporation
Electroporation involves the application of a high-voltage electric field to vegetative bacteria cells for a very short period. This technique resulted in major advances in genetic transformation of C. perfringens, due to the bacteria often displaying itself as a vegetative cell or as dormant spores in food.[23] The electric pulse creates pores in the bacterial cell membrane and allows the passive influx of DNA molecules.[24]
Metabolic processes
C. perfringens is an aerotolerant anaerobe bacterium that lives in a variety of environments including soil and human intestinal tract.[15]C. perfringens is incapable of synthesizing multiple amino acids due to the lack of genes required for biosynthesis.[15] Instead, the bacterium produces enzymes and toxins to break down host cells and import nutrients from the degrading cell.[15]
Membrane-damaging enzymes, pore-forming toxins, intracellular toxins, and hydrolytic enzymes are the functional categories into which C. perfringens' virulence factors may be divided. These virulence factor-encoding genes can be found on chromosomes and large plasmids.[26]
Carbohydrate-active enzymes
The human gastrointestinal tract is lined with intestinal mucosa that secrete mucus and act as a defense mechanism against pathogens, toxins, and harmful substances. Mucus is made up of mucins containing several O-linked glycanglycoproteins that recognizes and forms a barrier around microbes, preventing them from attaching to endothelial cells and infecting them.[27][28]C. perfringens can secrete different carbohydrate-active enzymes (CAZymes) that aid in degrading mucins and other O-glycans within the intestinal mucosa. These enzymes include: Sialidases, Hexosaminidases, Galactosidases, and Fucosidases belonging to various glycoside hydrolase families.[28]
Sialidase
Sialidases, also called neuraminidases, function to breakdown mucin by hydrolyzing the terminal sialic acid residues located within the protein through the process of desialylation. C. perfringens has three sialidases belonging to glycoside hydrolase family 33 (GH33): NanH, NanI, and NanJ. All strains of C. perfringens encode for at least one of these enzymes.[28][29]
C. perfringens can secrete NanI and NanJ through secretion signal peptides located on each protein. Research suggests that NanH operates in the cytoplasm of C. perfringens, as it does not contain a secretion signal peptide. NanH contains only a catalytic domain, whereas NanI and NanJ contain a catalytic domain and additional carbohydrate-binding modules (CBMs) to aid in catalytic activity. Located on their N-terminals, NanI contains CBM40, whereas NanJ contains both CBM40 and CBM32. Based on studies analyzing the three-dimensional structure of NanI, its active site has a pocket-like orientation that aids in the removal of sialic acid residues from sialomucins in the intestinal mucosa.[28]
Hexosaminidase
The mucus layer consists of intestinal mucin glycans, glycolipids, and glycoproteins that contain hexosamines, such as N-acetylglucosamine (GlcNAc) and N-acetylgalactosamine (GalNAc). C. perfringens encodes for eight hexosaminidases that break down hexosamines in the mucus. These hexosaminidases belong to four glycoside hydrolase families: GH36, GH84, GH89, and GH123.[28]
C. perfringens encodes for AagA (CpGH36A) and CpGH36B in glycoside hydrolase family 36 (GH36): AagA removes GalNAc from O-glycans, and CpGH36B is expected to have a similar structure to AagA, but specificities on its function are unknown. NagH, NagI, NagJ, and NagK, belonging to glycoside hydrolase family 84 (GH84), cleave terminal GlcNAc residues using a substrate-assisted digestion mechanism. AgnC (CpGH89), belonging to glycoside hydrolase family 89 (GH89), both cleaves GlcNAc from the ends of mucin glycans and acts on gastric mucin. Belonging to glycoside hydrolase family 123 (GH123), CpNga123 cleaves GalNAc, but research suggests that it only breaks down glycans taken up by C. perfringens due to the absence of a secretion signal peptide.[28]
Galactosidase
C. perfringens has four galactosidases that belong to the glycoside hydrolase family 2 (GH2): CpGH2A, CpGH2B, CpGH2C, and CpGH2D. Research suggests that these enzymes are effective at breaking down core mucin glycan structures with the ability to bind galactose using CBM51. However, minimal research exists on the specific functioning of galactosidases in C. perfringens.[28]
Fucosidase
Fucose monosaccharides are located on the terminal ends of core O-linked glycans. C. perfringens encodes for three fucosidases that belong to two glycoside hydrolase families: Afc1 and Afc2 in glycoside hydrolase family 29 (GH29), and Afc3 in glycoside hydrolase family 95 (GH95). Afc3 contains a C-terminal CBM51 and is the only fucosidase that contains a carbohydrate-binding module in C. perfringens. Fucosyl residues tend to cover the ends of glycans and protect them against enzymatic digestion, so research suggests that the ability of fucosidases to cleave complex and diverse fucosyl linkages is due to long-term adaptations in C. perfringens that persisted within close range of mucins.[28]
Major toxins
There are five major toxins produced by Clostridium perfringens. Alpha, beta, epsilon and enterotoxin are toxins that increase a cells permeability which causes an ion imbalance while iota toxins destroy the cell's actin cytoskeleton.[30] On the basis of which major, "typing" toxins are produced, C. perfringens can be classified into seven "toxinotypes", A, B, C, D, E, F and G:[31]
Alpha toxin (CPA) is a zinc-containing phospholipase C, composed of two structural domains, which destroy a cell's membrane. Alpha toxins are produced by all five types of C. perfringens. This toxin is linked to gas gangrene of humans and animals. Most cases of gas gangrene has been related to a deep wound being contaminated by soil that harbors C. perfringens.[30][33]
Beta toxin
Beta toxins (CPB) are a protein that causes hemorrhagic necrotizing enteritis and enterotoxaemia in both animals (type B) and humans (type C) which leads to the infected individual's feces becoming bloody and their intestines necrotizing.[30]Proteolytic enzymes, such as trypsin, can break down CPB, making them ineffective. Therefore, the presence of trypsin inhibitors in colostrum makes CPB especially deadly for mammal offspring.[34]
Epsilon toxin
Epsilon toxin (ETX) is a protein produced by type B and type D strains of C. perfringens. This toxin is currently ranked the third most potent bacterial toxin known.[35] ETX causes enterotoxaemia in mainly goats and sheep, but cattle are sometime susceptible to it as well. An experiment using mice found that ETX had an LD50 of 50-110ng/kg.[36] The excessive production of ETX increases the permeability of the intestines. This causes severe edema in organs such as the brain and kidneys.[37]
The very low LD50 of ETX has led to concern that it may be used as a bioweapon. It appeared on the select agent lists of the US CDC and USDA, until it was removed in 2012. There are no human vaccines for this toxin, but effective vaccines for animals exist.[38]
Iota toxin
Iota toxin (ITX) is a protein produced by type E strains of C. perfringens. Iota toxins are made up of two, unlinked proteins that form a multimeric complex on cells. Iota toxins prevent the formation of filamentous actin. This causes the destruction of the cells cytoskeleton which in turn leads to the death of the cell as it can no longer maintain homeostasis.[39]
Enterotoxin
This toxin (CPE) causes food poisoning. It alters intracellular claudin tight junctions in gut epithelial cells. This pore-forming toxin also can bind to human ileal and colonic epithelium in vitro and necrotize it. Through the caspase-3 pathway, this toxin can cause apoptosis of affected cells. This toxin is linked to type F strains, but has also been found to be produced by certain types of C, D, and E strains.[40]
Other toxins
TpeL is a toxin found in type B, C, and G[41] strains. It is in the same protein family as C. difficile toxin A.[42] It does not appear important in the pathogenesis of types B and C infections, but may contribute to virulence in type G strains. It glycosylates Rho and Ras GTPases, disrupting host cell signaling.[41]
Clostridium perfringens is a common cause of food poisoning in the United States. C. perfringens produces spores, and when these spores are consumed, they produce a toxin that causes diarrhea. Foods cooked in large batches and held at unsafe temperatures (between 40°F and 140°F) are the source of C. perfringens food poisoning outbreaks. Meats such as poultry, beef, and pork are commonly linked to C. perfringens food poisoning.[45]C. perfringens can proliferate in foods that are improperly stored due to the spore's ability to survive normal cooking temperatures. The type A toxin of C. perfringens, also known as the CPA is responsible for food poisoning.[46]
Clostridium perfringens is the most common bacterial agent for gas gangrene.[47] Gas gangrene is induced by α-toxin that embeds itself into the plasma membrane of cells and disrupts normal cellular function by altering membrane structure.[43] Some symptoms include blisters, tachycardia, swelling, and jaundice.[47]
C. perfringens is most commonly known for foodborne illness but can translocate from a gastrointestinal source into the bloodstream which causes bacteremia. C. perfringens bacteremia can lead to toxin-mediated intravascular hemolysis and septic shock.[48] This is rare as it makes up less than 1% of bloodstream isolates but is highly fatal with a reported mortality rate of 27% to 58%.[49]
Clostridium perfringens food poisoning can also lead to another disease known as enteritis necroticans or clostridial necrotizing enteritis, (also known as pigbel); this is caused by C. perfringens type C. This infection is often fatal. Large numbers of C. perfringens grow in the intestines and secrete exotoxin. This exotoxin causes necrosis of the intestines, varying levels of hemorrhaging, and perforation of the intestine. Inflammation usually occurs in sections of the jejunum, midsection of the small intestine.[50]Perfringolysin O (pfoA)-positive C. perfringens strains were also associated with the rapid onset of necrotizing enterocolitis in preterm infants.[51]
A strain of C. perfringens might be implicated in multiple sclerosis (MS) nascent (Pattern III) lesions.[52] Tests in mice found that two strains of intestinal C. perfringens that produced epsilon toxins (ETX) caused MS-like damage in the brain, and earlier work had identified this strain of C. perfringens in a human with MS.[53][54] MS patients were found to be 10 times more immune-reactive to the epsilon toxin than healthy people.[55]
Tissue gas occurs when C. perfringens infects corpses. It causes extremely accelerated decomposition and can only be stopped by embalming the corpse. Tissue gas most commonly occurs to those who have died from gangrene, large decubitus ulcers, necrotizing fasciitis or to those who had soil, feces, or water contaminated with C. perfringens forced into an open wound.[56]
Clinical Manifestations
Clostridium perfringens infections can lead to various clinical manifestations, ranging from mild gastrointestinal symptoms to life-threatening conditions. The most common presentation is food poisoning, characterized by acute abdominal pain, diarrhea, and, in some cases, vomiting, typically occurring 6 to 24 hours after the ingestion of contaminated food. Unlike many other foodborne illnesses, fever is usually absent. Symptoms are usually self-limiting and resolve within 24 to 48 hours; however, severe dehydration can occur in cases of significant fluid loss. Symptoms of dehydration include dry mouth, decreased urine output, dizziness, and fatigue. Severe symptoms such as diarrhea that persists for more than 48 hours, the inability to keep fluids down, or signs of severe dehydration may necessitate medical attention.[57] Most people are able to recover from C. perfringens food poisoning without treatment. However, people experience diarrhea are usually instructed to drink water or rehydration solutions.[58]
Gas gangrene caused by Clostridium perfringens is characterized by severe symptoms, including intense pain at the injury site, fever, rapid heart rate, sweating, and anxiety. The affected area may show signs of swelling, discoloration (ranging from pale to dark red or purplish), and large, discolored blisters filled with foul-smelling fluid. As the toxins spread, skin and muscle tissue are rapidly destroyed, leading to large areas of dead tissue, gas pockets under the skin (crepitus), and possible renal failure due to red blood cell destruction. Sepsis and septic shock may also occur, which can be fatal.[59]
Necrotizing enteritis caused by Clostridium perfringens presents with a wide range of symptoms, which can vary in severity. The clinical signs range from mild diarrhea to more severe manifestations such as intense abdominal pain, vomiting, bloody stools, and even septic shock. In the most serious cases, the infection can lead to death.[60]
Diagnosis
The diagnosis of Clostridium perfringens food poisoning relies on laboratory detection of the bacterium or its toxin in either a patient’s stool sample or contaminated food linked to the illness. A positive stool culture would have growth of at least 10 cfu/g of C. perfringens. Stool studies include WBCs, ova, and parasites in order to rule out other potential etiologies. ELISA testing is used to detect the CPA toxin. Diagnosing C. perfringens food poisoning is relatively uncommon for several reasons.[61] Most individuals with this foodborne illness do not seek medical care or submit a stool sample for testing, and routine testing for C. perfringens is not typically performed in clinical laboratories. Additionally, public health laboratories generally conduct testing for this pathogen only in the event of an outbreak.[62]
The diagnosis of gas gangrene typically involves several methods to confirm the infection. Imaging techniques such as X-rays, CT scans, or MRIs can reveal gas bubbles or tissue changes indicative of muscle damage. Additionally, bacterial staining or culture of fluid taken from the wound helps identify Clostridium perfringens and other bacteria responsible for the infection. In some cases, a biopsy is performed, where a sample of the affected tissue is analyzed for signs of damage or necrosis.[59]
The diagnosis of clostridial necrotizing enteritis is primarily based on the patient's clinical symptoms, which can include severe abdominal pain, vomiting, and bloody diarrhea. Additionally, confirmation of the presence of Clostridium perfringenstype C toxin in stool samples is crucial for accurate diagnosis.[60]
Epidemiology
Clostridium perfringens is responsible for an estimated 966,000 cases annually, or about 10.3% of all foodborne illnesses in which a pathogen is identified. Transmission typically occurs when food contaminated with C. perfringens spores is consumed, allowing the bacteria to produce a toxin in the intestines that causes diarrhea. Outbreaks are often associated with foods cooked in large batches, such as poultry, meat, and gravy, and held at unsafe temperatures between 40-140°F, which allows the bacteria to thrive. These outbreaks tend to occur in settings where large groups are served, such as hospitals, school cafeterias, prisons, nursing homes, and catered events. In most cases, C. perfringens infection causes mild symptoms, including watery diarrhea and mild abdominal cramps, with symptoms typically appearing 8 to 12 hours after consuming contaminated food and resolving within 24 hours. About 90% of affected individuals recover without seeking medical attention, usually within two days. However, vulnerable groups such as the elderly, young children, and immunocompromised individuals face a higher risk of severe complications like dehydration, which can lead to more serious illness or, in rare cases, death. Each year, C. perfringens infections result in approximately 438 hospitalizations and 26 deaths, accounting for 0.8% of foodborne illness-related hospitalizations and 1.9% of associated deaths. Outbreaks are most common in November and December, coinciding with holiday foods like turkey and roast beef. The economic burden of C. perfringens is significant, estimated at $342.7 million annually, including $53.2 million in medical costs, $64.3 million in productivity loss, and $225 million related to fatalities.[63][64]
Clostridial necrotizing enteritis is rare in the United States; typically, it occurs in populations with a higher risk. Data show that of the 9.4 million cases of foodborne illness in the United States each year, only about 11% are caused by Clostridium perfringens.[65] "Risk factors for enteritis necroticans include protein-deficient diet, unhygienic food preparation, sporadic feasts of meat (after long periods of a protein-deficient diet), diets containing large amounts of trypsin inhibitors (sweet potatoes), and areas prone to infection of the parasite Ascaris (produces a trypsin inhibitor). This disease is contracted in populations living in New Guinea, parts of Africa, Central America, South America, and Asia.[50]
Risk factors for gas gangrene include severe injuries, abdominal surgeries, and underlying health conditions such as colon cancer, diseases of the blood vessels, diabetes, and diverticulitis. However, the most common way to get gas gangrene is through a traumatic injury. In the United States, there is only about 1000 cases of gas gangrene per year. When addressed with adequate care, gas gangrene has a mortality rate of 20-30% but has a mortality rate of 100% if left untreated.[66]
Food poisoning incidents
On May 7, 2010, 42 residents and 12 staff members at a Louisiana (USA) state psychiatric hospital were affected and experienced vomiting, abdominal cramps, and diarrhea. Three patients died within 24 hours. The outbreak was linked to chicken which was cooked a day before it was served and was not cooled down according to hospital guidelines. The outbreak affected 31% of the residents of the hospital and 69% of the staff who ate the chicken. How many of the affected residents ate the chicken is unknown.[67]
In May 2011, a man died after allegedly eating food contaminated with the bacteria on a transatlanticAmerican Airlines flight. The man's wife and daughter were suing American and LSG Sky Chefs, the German company that prepared the inflight food.[68]
In December 2012, a 46-year-old woman died two days after eating a Christmas Day meal at a pub in Hornchurch, Essex, England. She was among about 30 people to fall ill after eating the meal. Samples taken from the victims contained C. perfringens. The hotel manager and the cook were jailed for forging cooking records relating to the cooking of the turkey.[69]
In December 2014, 87-year-old Bessie Scott died three days after eating a church potluck supper in Nackawic, New Brunswick, Canada. Over 30 other people reported signs of gastrointestinal illness, diarrhea, and abdominal pain. The province's acting chief medical officer says, Clostridium perfringens is the bacteria [sic] that most likely caused the woman's death.[70]
In October 2016, 66-year-old Alex Zdravich died four days after eating an enchilada, burrito, and taco at Agave Azul in West Lafayette, Indiana, United States. Three others who dined the same day reported signs of foodborne illness, which were consistent with the symptoms and rapid onset of C. perfringens infection. They later tested positive for the presence of the bacteria, but the leftover food brought home by Zdravich tested negative.[71][72]
In November 2016, food contaminated with C. perfringens caused three individuals to die, and another 22 to be sickened, after a Thanksgiving luncheon hosted by a church in Antioch, California, United States.[73]
In January 2017, a mother and her son sued a restaurant in Rochester, New York, United States, as they and 260 other people were sickened after eating foods contaminated with C. perfringens. "Officials from the Monroe County Department of Public Health closed down the Golden Ponds after more than a fourth of its Thanksgiving Day guests became ill. An inspection revealed a walk-in refrigerator with food spills and mold, a damaged gasket preventing the door from closing, and mildew growing inside."[74]
In July 2018, 647 people reported symptoms after eating at a Chipotle Mexican Grill restaurant in Powell, Ohio, United States. Stool samples tested by the CDC tested positive for C. perfringens.[75]
In November 2018, approximately 300 people in Concord, North Carolina, United States, were sickened by food at a church barbecue that tested positive for C. perfringens.[76]
In 2021, dozens of hospital workers in Alaska were sick and it was traced back to a Cubano Sandwich. Health officials wrote that almost all symptoms resolved within 24 hours. No one who ate the food reportedly needed hospitalization. It is rare for Alaska to see an outbreak with this magnitude when it's not associated with some sort of national food borne illness.[77]
Prevention
Preventing Clostridium perfringens contamination and growth involves careful food handling, proper cooking, and appropriate storage practices. Most foods, especially beef and chicken, can be protected by cooking them to the recommended internal temperatures. Using a kitchen thermometer is the most reliable way to check that meats reach safe cooking temperatures. As a general rule, food should be avoided if it smells, tastes, looks off, or has been left out at unsafe temperatures for a long period of time. [78]
C. perfringens spores can multiply within a temperature range of 59°F (15°C) to 122°F (50°C).[79] To prevent bacterial growth, leftovers should be refrigerated within two hours of preparation, with their temperature chilled down to below 40°F (4°C). Large portions of food that contain meat, should be divided into smaller containers before refrigeration to ensure even cooling. Before serving leftovers, they should be reheated to at least 165°F (74°C) to destroy any bacteria that may have grown during storage.[78]
High-risk foods, such as canned vegetables, smoked or cured meats, and salted or smoked fish, require additional attention. Improper processing or storage can allow bacteria to grow and produce dangerous toxins. Signs of contamination, such as unusual odors, changes in texture, or bulging cans (also known as "bombage"), indicate food spoilage and should be disposed.[80]
Preventing gas gangrene involves taking precautions to avoid bacterial infections. Healthcare providers follow strict protocols to prevent infections, including those caused by Clostridium perfringens. To reduce the risk of gas gangrene, individuals should clean wounds thoroughly with soap and water and seek medical attention for deep or uncleanable wounds. It is also essential to monitor injuries for changes in skin condition or the onset of severe pain. Wearing protective gear when engaging in activities like biking or motorcycling can help prevent injury. Additionally, working with healthcare providers to manage underlying conditions that affect circulation or weaken the immune system can further reduce the risk of infection.[59]
Treatment
The treatment of Clostridium perfringens infections depends on the type and severity of the condition. For severe infections, such as gas gangrene (clostridial myonecrosis), the primary approach involves surgical debridement of the affected area. This procedure removes devitalized tissue where bacteria grow, which limits the spread of the infection. Antimicrobial therapy is usually started at the same time, with penicillin being the most commonly used drug.[81] However, C. perfringens shows different resistance patterns with about 20% of strains being resistant to clindamycin, and 10% being resistant to metronidazole.[82]C. perfringens is often more susceptible to vancomycin when compared to other pathogenic Clostridia, making it an alternative option for treatment in some cases.[81]
Therapies, such as hyperbaric oxygen therapy (HBOT), may also be used for severe clostridial tissue infections. HBOT increases oxygen delivery to infected tissues, creating an environment that inhibits the growth of anaerobic bacteria like C. perfringens. While not commonly used, HBOT can be beneficial in certain cases.[83]
For foodborne illness caused by C. perfringens, treatment is typically unnecessary. Most people who suffer from food poisoning caused by C. perfringens usually fight off the illness without the need of any antibiotics. Extra fluids should be drank consistently until diarrhea dissipates.[84]
Research
C. perfringens has shown increasing multidrug resistance, particularly in strains from humans and animals. High resistance levels were found with antibiotics such as tetracycline, erythromycin, and sulfonamides. Genetic factors, misuse of antibiotics, and bacterial evolution are the cause of this issue. This highlights the importance of finding new treatment strategies.[85]
Multilocus Sequence Typing (MLST) and Whole Genome Sequencing (WGS) have been used to find the genetic diversity of C. perfringens. These methods have identified 195 distinct sequence types grouped into 25 clonal complexes from 322 genomes. Phylogenetic groups were also found in multiple different hosts and environmental sources. This highlights the bacteria's transmission potential and adaptability across species.[86]
Related Research Articles
Bacillus cereus is a Gram-positive rod-shaped bacterium commonly found in soil, food, and marine sponges. The specific name, cereus, meaning "waxy" in Latin, refers to the appearance of colonies grown on blood agar. Some strains are harmful to humans and cause foodborne illness due to their spore-forming nature, while other strains can be beneficial as probiotics for animals, and even exhibit mutualism with certain plants. B. cereus bacteria may be aerobes or facultative anaerobes, and like other members of the genus Bacillus, can produce protective endospores. They have a wide range of virulence factors, including phospholipase C, cereulide, sphingomyelinase, metalloproteases, and cytotoxin K, many of which are regulated via quorum sensing. B. cereus strains exhibit flagellar motility.
Clostridium botulinum is a gram-positive, rod-shaped, anaerobic, spore-forming, motile bacterium with the ability to produce botulinum toxin, which is a neurotoxin.
Gangrene is a type of tissue death caused by a lack of blood supply. Symptoms may include a change in skin color to red or black, numbness, swelling, pain, skin breakdown, and coolness. The feet and hands are most commonly affected. If the gangrene is caused by an infectious agent, it may present with a fever or sepsis.
Clostridium is a genus of anaerobic, Gram-positive bacteria. Species of Clostridium inhabit soils and the intestinal tracts of animals, including humans. This genus includes several significant human pathogens, including the causative agents of botulism and tetanus. It also formerly included an important cause of diarrhea, Clostridioides difficile, which was reclassified into the Clostridioides genus in 2016.
Foodborne illness is any illness resulting from the contamination of food by pathogenic bacteria, viruses, or parasites, as well as prions, and toxins such as aflatoxins in peanuts, poisonous mushrooms, and various species of beans that have not been boiled for at least 10 minutes.
An enterotoxin is a protein exotoxin released by a microorganism that targets the intestines. They can be chromosomally or plasmid encoded. They are heat labile, of low molecular weight and water-soluble. Enterotoxins are frequently cytotoxic and kill cells by altering the apical membrane permeability of the mucosal (epithelial) cells of the intestinal wall. They are mostly pore-forming toxins, secreted by bacteria, that assemble to form pores in cell membranes. This causes the cells to die.
The Clostridia are a highly polyphyletic class of Bacillota, including Clostridium and other similar genera. They are distinguished from the Bacilli by lacking aerobic respiration. They are obligate anaerobes and oxygen is toxic to them. Species of the class Clostridia are often but not always Gram-positive and have the ability to form spores. Studies show they are not a monophyletic group, and their relationships are not entirely certain. Currently, most are placed in a single order called Clostridiales, but this is not a natural group and is likely to be redefined in the future.
Gas gangrene is a bacterial infection that produces tissue gas in gangrene. This deadly form of gangrene usually is caused by Clostridium perfringens bacteria. About 1,000 cases of gas gangrene are reported yearly in the United States.
Clostridial necrotizing enteritis (CNE) is a severe and potentially fatal type of food poisoning caused by a β-toxin of Clostridium perfringens, Type C. It occurs in some developing regions, particularly in New Guinea, where it is known as pig-bel. The disease was also documented in Germany following World War II, where it was called Darmbrand (literally "bowel fire," or bowel necrosis). The toxin is normally inactivated by certain proteolytic enzymes and by normal cooking, but when these protections are impeded by diverse factors, and high protein is consumed, the disease can emerge.
Clostridium perfringens alpha toxin is a toxin produced by the bacterium Clostridium perfringens and is responsible for gas gangrene and myonecrosis in infected tissues. The toxin also possesses hemolytic activity.
Clostridium septicum is a gram positive, spore forming, obligate anaerobic bacterium.
Clostridium enterotoxins are toxins produced by Clostridium species. Clostridial species are one of the major causes of food poisoning/gastrointestinal illnesses. They are anaerobic, gram-positive, spore-forming rods that occur naturally in the soil. Among the family are: Clostridium botulinum, which produces one of the most potent toxins in existence; Clostridium tetani, causative agent of tetanus; and Clostridium perfringens, commonly found in wound infections and diarrhea cases.
Microbial toxins are toxins produced by micro-organisms, including bacteria, fungi, protozoa, dinoflagellates, and viruses. Many microbial toxins promote infection and disease by directly damaging host tissues and by disabling the immune system. Endotoxins most commonly refer to the lipopolysaccharide (LPS) or lipooligosaccharide (LOS) that are in the outer plasma membrane of Gram-negative bacteria. The botulinum toxin, which is primarily produced by Clostridium botulinum and less frequently by other Clostridium species, is the most toxic substance known in the world. However, microbial toxins also have important uses in medical science and research. Currently, new methods of detecting bacterial toxins are being developed to better isolate and understand these toxins. Potential applications of toxin research include combating microbial virulence, the development of novel anticancer drugs and other medicines, and the use of toxins as tools in neurobiology and cellular biology.
Clostridium novyi (oedematiens) a Gram-positive, endospore- forming, obligate anaerobic bacteria of the class Clostridia. It is ubiquitous, being found in the soil and faeces. It is pathogenic, causing a wide variety of diseases in humans and animals.
Clostridium perfringens beta toxin is one of the four major lethal protein toxins produced by Clostridium perfringens Type B and Type C strains. It is a necrotizing agent and it induces hypertension by release of catecholamine. It has been shown to cause necrotic enteritis in mammals and induces necrotizing intestinal lesions in the rabbit ileal loop model. C. perfringens beta toxin is susceptible to breakdown by proteolytic enzymes, particularly trypsin. Beta toxin is therefore highly lethal to infant mammals because of trypsin inhibitors present in the colostrum.
Hathewaya histolytica is a species of bacteria found in feces and the soil. It is a motile, gram-positive, aerotolerant anaerobe. H. histolytica is pathogenic in many species, including guinea pigs, mice, and rabbits, and humans. H. histolytica has been shown to cause gas gangrene, often in association with other bacteria species.
Clostridium innocuum is an anaerobic, non-motile, gram-positive bacterium that reproduces by sporulation. While there are over 130 species of Clostridium, C. innocuum is the third most commonly isolated. Although it is not normally considered an aggressive human pathogen, it has been isolated in some disease processes. C. innocuum and other Clostridium line the oropharynx and gastrointestinal tract, and are considered normal gut flora.
Clostridium tertium is an anaerobic, motile, gram-positive bacterium. Although it can be considered an uncommon pathogen in humans, there has been substantial evidence of septic episodes in human beings. C. tertium is easily decolorized in Gram-stained smears and can be mistaken for a Gram-negative organism. However, C.tertium does not grow on selective media for Gram-negative organisms.
In molecular biology, VR-RNA is a small RNA produced by Clostridium perfringens. It functions as a regulator of the two-component VirR/VirS system.
Clostridioides difficile is a bacterium known for causing serious diarrheal infections, and may also cause colon cancer. It is known also as C. difficile, or C. diff, and is a Gram-positive species of spore-forming bacteria. Clostridioides spp. are anaerobic, motile bacteria, ubiquitous in nature and especially prevalent in soil. Its vegetative cells are rod-shaped, pleomorphic, and occur in pairs or short chains. Under the microscope, they appear as long, irregular cells with a bulge at their terminal ends. Under Gram staining, C. difficile cells are Gram-positive and show optimum growth on blood agar at human body temperatures in the absence of oxygen. C. difficile is catalase- and superoxide dismutase-negative, and produces up to three types of toxins: enterotoxin A, cytotoxin B and Clostridioides difficile transferase. Under stress conditions, the bacteria produce spores that are able to tolerate extreme conditions that the active bacteria cannot tolerate.
References
↑ Ryan, Kenneth J.; Ray, C. George (2004). Sherris Medical Microbiology: an Introduction to Infectious Diseases (4thed.). New York: McGraw-Hill. p.310. ISBN978-0-8385-8529-0.
↑ Juckett, G; Bardwell, G; McClane, B; Brown, S (2008). "Microbiology of salt rising bread". The West Virginia Medical Journal. 104 (4): 26–7. PMID18646681.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.