ABSTRACT
Background: Cirrhosis is a prevalent disease and ranks among the leading causes of death worldwide. Sarcopenia is believed to be associated with a poorer prognosis in patients with cirrhosis.
Objective: To evaluate the impact of sarcopenia on the prognosis of patients hospitalized for acute decompensation of cirrhosis, with or without acute-on-chronic liver failure.
Methods: This prospective cohort study evaluated patients hospitalized for acute decompensation of cirrhosis, with or without acute-on-chronic liver failure. Sarcopenia was assessed according to the European Working Group on Sarcopenia in Older People, using skeletal muscle mass analysis by bioelectrical impedance and handgrip strength testing. The data was collected between March-2019 and April-2020. Qualitative variables were presented as frequencies and percentages, and quantitative variables as means and standard deviations when symmetrical, or medians and 25th and 75th percentiles when asymmetrical. The association of sarcopenia and mortality with quantitative variables was tested using Student’s t-test or the Mann-Whitney test, while associations with qualitative variables were tested using the Chi-square test or Fisher’s Exact test. For significant associations, crude and adjusted (multivariate analysis) relative risk estimates with a 95% confidence interval were calculated using Poisson regression analysis. Results with P<0.05 were considered significant.
Results: Fifty patients were included, with a mean age of 60.5 years (±10.4) and a slight predominance of men (56%). The main causes of cirrhosis were alcohol use disorder (28%) and hepatitis C (24%). The median Child-Pugh score was 8 points (7-10), and the median Model for End-stage Liver Disease score was 15 points (12.5-21). Ten patients were diagnosed with acute-on-chronic liver failure. Sarcopenia was present in 50% of the sample. Sarcopenia was present in 70.0% of patients with acute-on-chronic liver failure and in 43.2% of those without acute-on-chronic liver failure (P=0.168). Overall mortality was 48% in patients with sarcopenia and 44% in those without sarcopenia (P=1.000). In multivariate analysis, overall mortality was associated only with leukocyte count (relative risk=1.01, 95% confidence interval=1.01-1.01) and Model for End-stage Liver Disease score (relative risk=1.07, 95% confidence interval =1.03-1.10).
Conclusion: In this study, sarcopenia was not associated with mortality in patients hospitalized for acute decompensation of cirrhosis, with or without acute-on-chronic liver failure. There was a non-significant trend towards a higher prevalence of sarcopenia among individuals with acute-on-chronic liver failure.
Keywords: Cirrhosis; sarcopenia; acute decompensation; acute-on-chronic liver failure; mortality
RESUMO
Contexto: A cirrose é uma doença prevalente e está entre as principais causas de óbito internacionalmente. Acredita-se que a sarcopenia possa estar associada a um pior prognóstico em pacientes com cirrose.
Objetivo: Avaliar o impacto da sarcopenia no prognóstico de pacientes hospitalizados por descompensação aguda da cirrose, com ou sem falência hepática crônica agudizada.
Métodos: Este estudo de coorte prospectivo avaliou pacientes hospitalizados por descompensação aguda da cirrose, com ou sem falência hepática crônica agudizada. A sarcopenia foi avaliada de acordo com o European Working Group on Sarcopenia in Older People, com análise da massa muscular esquelética por bioimpedância elétrica e com a aferição da força pelo teste da preensão palmar. Os dados foram coletados entre março de 2019 e abril de 2020. Variáveis qualitativas foram apresentadas como frequências e percentuais, e as quantitativas, como médias e desvios-padrão, quando simétricas, ou como medianas e percentis 25% e 75%, quando assimétricas. A associação de sarcopenia e de óbito com as variáveis quantitativas foi verificada pelo teste t de Student ou pelo teste de Mann-Whitney, enquanto tais associações com variáveis qualitativas foram verificadas pelo teste Qui-Quadrado ou pelo teste Exato de Fisher. Para as associações significativas, foram calculadas as estimativas bruta e ajustada (análise multivariada) de risco relativo com intervalo de confiança de 95% através da análise de regressão de Poisson. Foram considerados significativos os resultados com P<0,05.
Resultados: Foram incluídos 50 pacientes, com média de idade de 60,5 anos (±10,4) e um discreto predomínio de homens (56%). As principais causas de cirrose foram o consumo problemático de álcool (28%) e a hepatite C (24%). O escore de Child-Pugh mediano foi de 8 pontos (7-10), e o escore Model for End-stage Liver Disease mediano foi de 15 pontos (12,5-21). Dez pacientes tiveram diagnóstico de falência hepática crônica agudizada. Sarcopenia esteve presente em 50% da amostra. A sarcopenia esteve presente em 70,0% dos pacientes com falência hepática crônica agudizada e em 43,2% daqueles sem falência hepática crônica agudizada (P=0,168). A mortalidade geral foi de 48% nos pacientes com sarcopenia e de 44% naqueles sem sarcopenia (P=1,000). Na análise multivariada, a mortalidade geral esteve associada apenas à contagem de leucócitos (risco relativo=1,01, intervalo de confiança de 95%=1,01-1,01) e ao escore Model for End-stage Liver Disease (risco relativo=1,07, intervalo de confiança de 95%=1,03-1,10).
Conclusão: Neste estudo, a sarcopenia não esteve associada à mortalidade dos pacientes internados por descompensação aguda da cirrose, com ou sem falência hepática crônica agudizada. Houve uma tendência não significativa a uma maior prevalência de sarcopenia em indivíduos com falência hepática crônica agudizada.
Palavras-chave: Cirrose; sarcopenia; descompensação aguda; acute-on-chronic liver failure; mortalidade
HIGHLIGHTS
•The study aimed to evaluate the impact of sarcopenia on the prognosis of patients hospitalized for acute decompensation of cirrhosis, with or without ACLF.
•This prospective cohort study assessed for sarcopenia based on bioelectrical impedance and handgrip strength testing.
•There was a trend towards a higher prevalence of sarcopenia among individuals with ACLF.
•Sarcopenia was not associated with mortality in patients hospitalized for acute decompensation of cirrhosis, with or without ACLF.
INTRODUCTION
Cirrhosis is a disease that has a high impact and cost on the healthcare system, in addition to having high mortality rates. In the economic side, according to the Global Burden of Disease, cirrhosis has higher costs than almost all other liver diseases, and high rates of readmissions due to the inherent decompensation in these patients1. Regarding mortality rates, it is the seventh leading cause of deaths among adults in the world, most of deaths being related to acute decompensation and acute-on-chronic liver failure (ACLF)2,3.
According to several studies4-7, sarcopenia may be associated with the prognosis of individuals with liver diseases. This syndrome, initially described in the older people8, is characterized by the progressive and generalized loss of muscle mass and function, and is currently being studied for its relation to several other conditions beyond liver diseases4,5, such as pulmonary, renal, and cardiac diseases9-11. Some studies report higher mortality rates among patients on the liver transplant waiting list when sarcopenia is present; a higher prevalence of ACLF among patients with sarcopenia; and higher rates of metabolic dysfunction-associated steatotic liver disease (MASLD) in individuals with sarcopenia12-14.
However, there are only a few studies that evaluate sarcopenia in patients with cirrhosis and ACLF, indicating the need for further studies that can shed light on this topic. Thus, the present study aims to evaluate the presence of an association between sarcopenia and mortality among patients hospitalized for acute decompensation of cirrhosis, with or without ACLF.
METHODS
Design
A prospective cohort study was conducted with patients hospitalized for acute decompensation of cirrhosis at a tertiary hospital in southern Brazil. Data were collected from a sample composed of all consecutive patients who met the eligibility criteria between April 2019 and March 2020. The study was written based on the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE).
Eligibility criteria
Patients with liver cirrhosis hospitalized for acute decompensation of the disease (development of ascites, hepatic encephalopathy, gastrointestinal bleeding, or infection) were included. Patients under 18 years of age, pregnant women, and patients with hepatocellular carcinoma exceeding the Milan criteria (advanced hepatocellular carcinoma) or with other extrahepatic malignancies in the 2 years preceding the study were excluded. Pacemaker users were also excluded due to a contraindication for performing bioelectrical impedance analysis in such patients.
Sarcopenia assessment
As there are no specific parameters in the literature for patients with liver diseases, the criteria and cut-off points of the Revised European Consensus on Sarcopenia, from the European Working Group on Sarcopenia in Older People (EWGSOP2)8, the most widely accepted reference for the diagnosis of the syndrome, were adopted. All evaluations were conducted by the same professional, previously trained for the research parameters.
Muscle strength was measured by handgrip strength (Smedley Spring, Baseline, New York, USA), following the recommendations of the American Society of Hand Therapy15. The adopted cut-off points were <16 kg/f for women and <27 kg/f for men. Skeletal muscle mass (SMM) was assessed by bioelectrical impedance analysis (Maltron BF-906 Body Fat Analyzer, Maltron International Ltd., Essex, UK). Patient preparation followed the recommendations of the European Society for Clinical Nutrition and Metabolism16. Bioimpedance resistance was collected and applied to the formula proposed by Janssen et al.17. The adopted cut-off point was SMM <20 kg/m² for men and <15 kg/m² for women.
Other variables
Demographic, clinical, and laboratory variables that could influence the prognosis were also evaluated. Variables were assessed at the time of hospital admission. These variables included the etiology of cirrhosis, reason for hospitalization, history of previous hospitalizations for acute decompensations of cirrhosis, alcohol consumption in the three months preceding hospitalization, bilirubin, albumin, prothrombin time through the international normalized ratio (INR), presence of hepatic encephalopathy (according to the West Haven criteria), presence and grade of ascites, use of vasopressors, need for dialysis, need for mechanical ventilation, partial oxygen saturation/inspired oxygen fraction ratio, Child-Pugh score, Model for End-stage Liver Disease (MELD) score, MELD-sodium score, and presence of ACLF. The diagnosis of ACLF was made according to the criteria proposed by the Chronic Liver Failure Consortium (CLIF-C), based on the CANONIC study18.
Ethical aspects
The research followed all ethical norms and guidelines, complying with the resolution of the National Health Council number 466/12. All participants signed the Informed Consent Form (ICF), and the project was approved by the institutional review board under number 06129718.6.1001.5335.
Statistical analysis
The results of qualitative variables were presented as frequencies and percentages, while those of quantitative variables were presented as means and standard deviations when symmetrical, or as medians and 25% and 75% percentiles when asymmetrical. The normality of the variables was verified by the Shapiro-Wilk test.
The association of sarcopenia and death with quantitative variables was verified by Student’s t-test or the Mann-Whitney test, according to the distribution of the variables, while such associations with qualitative variables were verified by the Chi-Square test or Fisher’s Exact test. For significant associations, the crude and adjusted (multivariate) relative risk (RR) estimates with a 95% confidence interval (95%CI) were calculated using Poisson regression analysis with robust variance adjustment. Results with a p-value <0.05 were considered significant. The analyses were performed using the statistical software SPSS 25.0 (IBM SPSS Statistics for Windows, Armonk, New York, USA).
RESULTS
Fifty patients were included, with a mean age of 60.5 years (±10.4) and a slight predominance of men (56%). The main causes of cirrhosis were alcohol use disorder (28%) and hepatitis C (24%). Most of the patients had ascites (76% of the sample). The median Child-Pugh score of the patients was 8 points (7;10). The median MELD score of the patients was 15 points (12.5;21). Ten patients had ACLF. The baseline characteristics of the studied population are presented in Table 1 (categorical variables) and Table 2 (continuous variables).
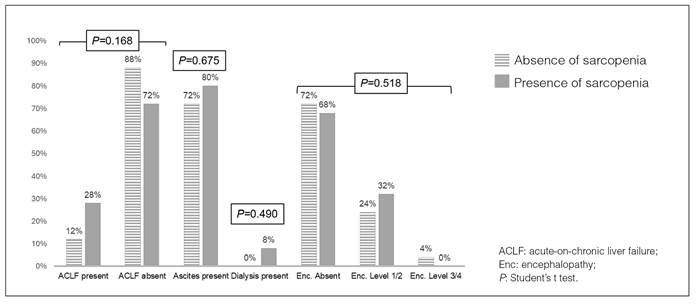
Sarcopenia was present in 50% of the sample. The proportion of women was significantly higher among patients with sarcopenia compared to that of those without this condition (72% versus 16%, P<0.001). Handgrip strength and SMM were significantly lower among patients with sarcopenia compared to their counterparts, as expected considering the diagnostic criteria of the syndrome. There were no other significant differences between the baseline characteristics of patients with and without sarcopenia. It was observed a non-significant trend towards a higher prevalence of sarcopenia among individuals with ACLF compared to those without ACLF (70.0% versus 43.2%, P=0.168). The differences between patients with and without sarcopenia regarding ACLF, ascites, dialysis and encephalopathy can be seen in Figure 1.

Mortality was 12% at 28 days and 22% at 90 days, with an overall mortality of 46% at the end of the follow-up period. When comparing patients with or without sarcopenia, 28-day mortality was 12% for both groups (P=1.000). However, 90-day mortality was 20% for patients with sarcopenia and 24% for those without (P=1.000). Finally, overall mortality was 48% for individuals with sarcopenia and 44% for patients without sarcopenia (P=1.000).
In the univariate analysis, the presence of ACLF, presence of ascites, length of hospital stay, bilirubin levels, INR, creatinine levels, leukocyte count, and C-reactive protein, as well as Child-Pugh, MELD, and MELD-sodium scores, were potentially associated with overall mortality (P<0.1). Sarcopenia was not associated with overall mortality (P=1.000). In the multivariate analysis, the only variables independently associated with overall mortality were leukocyte count (RR=1.01, 95% CI=1.01-1.01, P<0.001) and MELD score (RR=1.07, 95% CI=1.03-1.10, P<0.001). For every increase of 1000 leukocytes, the risk of death increased by 1%. Regarding the MELD score, for every 1-point increase in the score, the risk of death increased by 7% in the multivariate analysis. The univariate and multivariate analyses are presented in Table 3.
DISCUSSION
This prospective cohort study assessed the impact of sarcopenia in the prognosis of patients hospitalized for acute decompensation of cirrhosis, with or without ACLF. No significant association was found between the presence of sarcopenia and the mortality of these patients. Although there was a trend towards an association between sarcopenia and ACLF, it was not statistically significant.
Sarcopenia was originally described as a syndrome affecting the older people8. However, it is currently the focus of several studies in various populations with chronic diseases, such as liver4,5, heart9 and renal diseases10, and it is also associated with other syndromes or conditions, such as obesity19,20, osteoporosis21, and frailty22.
The current concept of this syndrome includes the evaluation of muscle mass combined with the evaluation of muscle function (strength and performance)8, but most of the evidence related to patients with sarcopenia associated with cirrhosis is limited to the assessment of muscle mass only23. In this study, we sought to evaluate not only muscle mass but also strength, combining two parameters, which is considered essential for the diagnostic definition of sarcopenia8.
In our study, sarcopenia was found in 50% of the studied population, which is consistent with the study by Romagna et al. (49.4%)24. However, the prevalence of sarcopenia in cirrhosis can vary widely7,25, likely due to the different methods and cut-off points used in the definition of sarcopenia in cirrhosis, as well as the stage of the natural history of the disease when patients were evaluated6.
Mortality was similar in patients with and without sarcopenia in this study. The impact of sarcopenia on the survival of patients with cirrhosis remains controversial, with some studies demonstrating an association between sarcopenia and lower survival in this patient population23,26,27. However, these studies defined sarcopenia based solely on the assessment of muscle mass and did not evaluate muscle strength, which could explain some differences compared to the present study. On the other hand, a meta-analysis was unable to demonstrate evidence that sarcopenia significantly increased the mortality of patients with cirrhosis on the transplant waiting list, showing only a significant association between sarcopenia and post-transplant mortality28.
Despite the higher prevalence of sarcopenia among individuals with ACLF, no significant association was found between these conditions in the present study. This contradicts the findings of a recent study that identified sarcopenia as an independent risk factor for the development of ACLF26. That may be due to a lack of statistical power of the present study to identify such an association.
The importance of systemic inflammation in the pathophysiology of decompensation of cirrhosis and ACLF is currently recognized12,14. In this study, the only two factors independently associated with mortality were the MELD score, traditionally associated with lower survival rates among patients with cirrhosis29, and leukocyte count, precisely a marker associated with systemic inflammation18.
Regarding the evaluation of sarcopenia, methods recommended by the EWGSOP were used in our study8. Although international guidelines on sarcopenia in cirrhosis identify the tomographic evaluation of the psoas muscle at the level of the L3 vertebra as the gold standard for diagnosing muscle mass loss, they also recognize that the technique has little clinical applicability due to high cost and radiation exposure29, and alone, this assessment is not sufficient to adequately diagnose the syndrome8. For this reason, we chose to evaluate sarcopenia in this study by combining the assessment of muscle strength by the handgrip strength test and skeletal muscle mass by bioelectrical impedance analysis, making it more difficult to compare our results to those of other studies.
It is also important to highlight that there is still a discussion in the literature on sarcopenia about tests for diagnosing sarcopenia, mainly strength and physical performance tests30. Patients with compromised mobility or other severe limitations, such as frail patients, octogenarians and nonagenarians, or those with chronic diseases, such as advanced liver disease, may be underestimated in these tests31. Therefore, a discussion in the specific literature on the most accurate tests for detecting sarcopenia in this type of population is also necessary.
As limitations of this study, we can highlight the small sample size, which may have hidden some significant correlations that might have been identified with a larger sample. Moreover, it could be argued that bioelectrical impedance analysis might underestimate the presence of sarcopenia in patients with edema or ascites32. The measurement of the phase angle could be helpful and does not seem to be substantially impacted by the presence of ascites23, but unfortunately this resource was unavailable in our equipment. It is important to emphasize, however, that bioelectrical impedance analysis, even without the phase angle measurement, has been successfully used in assessing sarcopenia in patients with cirrhosis, including those with ascites33.
In conclusion, in the present study, sarcopenia was not associated with the mortality of patients hospitalized for acute decompensation of cirrhosis, with or without ACLF, nor was it significantly associated with the presence of ACLF. We believe that more studies with a larger number of participants and using techniques for evaluating sarcopenia recommended by the main guidelines in the literature are necessary to better understand the impact of sarcopenia on cirrhosis.
ACKNOWLEDGEMENTS
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001 (scholarship granted to Eifler LM; and PhD fellowship granted to Ferreira LF).
REFERENCES
- 1 GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396:1204-22.
- 2 Moon AM, Singal AG, Tapper EB. Contemporary Epidemiology of Chronic Liver Disease and Cirrhosis. Clin Gastroenterol Hepatol. 2020;18:2650-66.
- 3 Nader LA, de Mattos AA, Bastos GA. Burden of liver disease in Brazil. Liver Int. 2014;34:844-9.
- 4 Perisetti A, Goyal H, Yendala R, Chandan S, Tharian B, Thandassery RB. Sarcopenia in hepatocellular carcinoma: Current knowledge and future directions. World J Gastroenterol. 2022;28:432-48.
- 5 Chun HS, Kim MN, Lee JS, Lee HW, Kim BK, Park JY, et al. Risk stratification using sarcopenia status among subjects with metabolic dysfunction-associated fatty liver disease. J Cachexia Sarcopenia Muscle. 2021;12:1168-78.
- 6 Bhanji RA, Saiman Y, Watt KD. Nonalcoholic Steatohepatitis, Sarcopenia, and Liver Transplantation. Clin Liver Dis. 2021;17:2-5.
- 7 Ebadi M, Bhanji RA, Mazurak VC, Montano-Loza AJ. Sarcopenia in cirrhosis: from pathogenesis to interventions. J Gastroenterol. 2019;54:845-59.
- 8 Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48:16-31.
- 9 Ebner N, von Haehling S. [Cachexia and sarcopenia in chronic heart failure: Change in muscle strength and muscle structure]. Internist (Berl). 2018;59:439-44.
- 10 Gungor O, Ulu S, Hasbal NB, Anker SD, Kalantar-Zadeh K. Effects of hormonal changes on sarcopenia in chronic kidney disease: where are we now and what can we do? J Cachexia Sarcopenia Muscle. 2021;12:1380-92.
- 11 Ohara DG, Pegorari MS, Oliveira Dos Santos NL, de Fátima Ribeiro Silva C, Oliveira MSR, Matos AP, et al. Cross-Sectional Study on the Association between Pulmonary Function and Sarcopenia in Brazilian Community-Dwelling Elderly from the Amazon Region. J Nutr Health Aging. 2020;24:181-7.
- 12 Arroyo V, Moreau R, Jalan R, Ginès P. Acute-on-chronic liver failure: A new syndrome that will re-classify cirrhosis. J Hepatol. 2015;62(1 Suppl):S131-43.
- 13 Carey EJ, Lai JC, Wang CW, Dasarathy S, Lobach I, Montano-Loza AJ, et al. A multicenter study to define sarcopenia in patients with end-stage liver disease. Liver Transpl. 2017;23:625-33.
- 14 Trebicka J, Fernandez J, Papp M, Caraceni P, Laleman W, Gambino C, et al. The PREDICT study uncovers three clinical courses of acutely decompensated cirrhosis that have distinct pathophysiology. J Hepatol. 2020;73:842-54.
- 15 Fess E. Grip Strength. In: Clinical assessment recommendations. Therapists ASoH, editor. Chicago, IL: JS C, editor. ; 1992.
- 16 Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P, Elia M, Manuel Gómez J, et al. Bioelectrical impedance analysis-part II: utilization in clinical practice. Clin Nutr. 2004;23:1430-53.
- 17 Janssen I, Heymsfield SB, Baumgartner RN, Ross R. Estimation of skeletal muscle mass by bioelectrical impedance analysis. J Appl Physiol. 2000;89:465-71.
- 18 Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013;144:1426-37,37.e1-9.
- 19 Balachandran A, Krawczyk SN, Potiaumpai M, Signorile JF. High-speed circuit training vs hypertrophy training to improve physical function in sarcopenic obese adults: a randomized controlled trial. Exp Gerontol. 2014;60:64-71.
- 20 Choi KM. Sarcopenia and sarcopenic obesity. Korean J Intern Med. 2016;31:1054-60.
- 21 Petermann-Rocha F, Ferguson LD, Gray SR, Rodríguez-Gómez I, Sattar N, Siebert S, et al. Association of sarcopenia with incident osteoporosis: a prospective study of 168,682 UK biobank participants. J Cachexia Sarcopenia Muscle. 2021;12:1179-88.
- 22 Cadore EL, Rodríguez-Mañas L, Sinclair A, Izquierdo M. Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: a systematic review. Rejuvenation Res. 2013;16:105-14.
- 23 Ruiz-Margáin A, Xie JJ, Román-Calleja BM, Pauly M, White MG, Chapa-Ibargüengoitia M, et al. Phase Angle From Bioelectrical Impedance for the Assessment of Sarcopenia in Cirrhosis With or Without Ascites. Clin Gastroenterol Hepatol. 2021;19:1941-9.e2.
- 24 Romagna ES, Appel-da-Silva MC, Suwa E, Maeda FK, Mattos AA, Tovo CV. Muscle depletion in cirrhotic patients assessed using computed tomography: a cross-sectional study. Sao Paulo Med J. 2020;138:152-7.
- 25 Kim G, Kang SH, Kim MY, Baik SK. Prognostic value of sarcopenia in patients with liver cirrhosis: A systematic review and meta-analysis. PloS one. 2017;12:e0186990.
- 26 Mauro E, Crespo G, Martinez-Garmendia A, Gutierrez-Acevedo MN, Diaz JM, Saidman J, et al. Cystatin C and Sarcopenia Predict Acute on Chronic Liver Failure Development and Mortality in Patients on the Liver Transplant Waiting List. Transplantation. 2020;104(7):e188-e98.
- 27 Hara N, Iwasa M, Sugimoto R, Mifuji-Moroka R, Yoshikawa K, Terasaka E, et al. Sarcopenia and Sarcopenic Obesity Are Prognostic Factors for Overall Survival in Patients with Cirrhosis. Intern Med. 2016;55:863-70.
- 28 Al-Judaibi B, Alqalami I, Sey M, Qumosani K, Howes N, Sinclair L, et al. Exercise Training for Liver Transplant Candidates. Transplant Proc. 2019;51:3330-7.
- 29 Lai JC, Tandon P, Bernal W, Tapper EB, Ekong U, Dasarathy S, et al. Malnutrition, Frailty, and Sarcopenia in Patients With Cirrhosis: 2021 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology. 2021;74:1611-44.
- 30 Ferreira LF, Scariot EL, da Rosa LHT. The effect of different exercise programs on sarcopenia criteria in older people: A systematic review of systematic reviews with meta-analysis. Arch Gerontol Geriatr. 2023;105:104868.
- 31 Morley JE, Abbatecola AM, Argiles JM, Baracos V, Bauer J, Bhasin S, et al. Sarcopenia with limited mobility: an international consensus. J Am Med Dir Assoc. 2011;12:403-9.
- 32 European Association for the Study of the Liver. EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J Hepatol. 2019;70:172-93.
- 33 Praktiknjo M, Book M, Luetkens J, Pohlmann A, Meyer C, Thomas D, et al. Fat-free muscle mass in magnetic resonance imaging predicts acute-on-chronic liver failure and survival in decompensated cirrhosis. Hepatology. 2018;67:1014-26.
Publication Dates
-
Publication in this collection
25 Nov 2024 -
Date of issue
2024
History
-
Received
11 July 2024 -
Accepted
17 Sept 2024