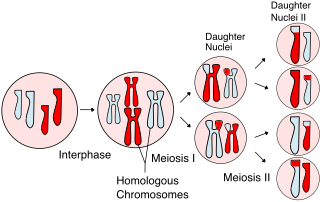
Meiosis (; from Ancient Greek μείωσις 'lessening', is a special type of cell division of germ cells in sexually-reproducing organisms that produces the gametes, the sperm or egg cells. It involves two rounds of division that ultimately result in four cells, each with only one copy of each chromosome. Additionally, prior to the division, genetic material from the paternal and maternal copies of each chromosome is crossed over, creating new combinations of code on each chromosome. Later on, during fertilisation, the haploid cells produced by meiosis from a male and a female will fuse to create a zygote, a cell with two copies of each chromosome again.

A testicle or testis is the male gonad in all bilaterians, including humans. It is homologous to the female ovary. The functions of the testicles are to produce both sperm and androgens, primarily testosterone. Testosterone release is controlled by the anterior pituitary luteinizing hormone, whereas sperm production is controlled both by the anterior pituitary follicle-stimulating hormone and gonadal testosterone.

A gonad, sex gland, or reproductive gland is a mixed gland and sex organ that produces the gametes and sex hormones of an organism. Female reproductive cells are egg cells, and male reproductive cells are sperm. The male gonad, the testicle, produces sperm in the form of spermatozoa. The female gonad, the ovary, produces egg cells. Both of these gametes are haploid cells. Some hermaphroditic animals have a type of gonad called an ovotestis.
Gametogenesis is a biological process by which diploid or haploid precursor cells undergo cell division and differentiation to form mature haploid gametes. Depending on the biological life cycle of the organism, gametogenesis occurs by meiotic division of diploid gametocytes into various gametes, or by mitosis. For example, plants produce gametes through mitosis in gametophytes. The gametophytes grow from haploid spores after sporic meiosis. The existence of a multicellular, haploid phase in the life cycle between meiosis and gametogenesis is also referred to as alternation of generations.
A germ cell is any cell that gives rise to the gametes of an organism that reproduces sexually. In many animals, the germ cells originate in the primitive streak and migrate via the gut of an embryo to the developing gonads. There, they undergo meiosis, followed by cellular differentiation into mature gametes, either eggs or sperm. Unlike animals, plants do not have germ cells designated in early development. Instead, germ cells can arise from somatic cells in the adult, such as the floral meristem of flowering plants.

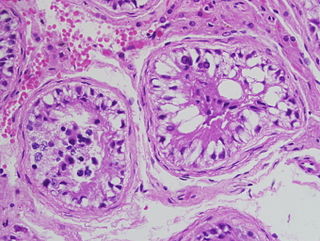
Seminiferous tubules are located within the testicles, and are the specific location of meiosis, and the subsequent creation of male gametes, namely spermatozoa.
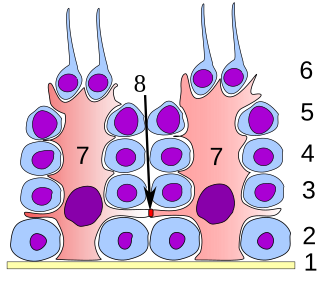
Sertoli cells are a type of sustentacular "nurse" cell found in human testes which contribute to the process of spermatogenesis as a structural component of the seminiferous tubules. They are activated by follicle-stimulating hormone (FSH) secreted by the adenohypophysis and express FSH receptor on their membranes.
The spermatid is the haploid male gametid that results from division of secondary spermatocytes. As a result of meiosis, each spermatid contains only half of the genetic material present in the original primary spermatocyte.

Spermatocytes are a type of male gametocyte in animals. They derive from immature germ cells called spermatogonia. They are found in the testis, in a structure known as the seminiferous tubules. There are two types of spermatocytes, primary and secondary spermatocytes. Primary and secondary spermatocytes are formed through the process of spermatocytogenesis.
Reproductive biology includes both sexual and asexual reproduction.
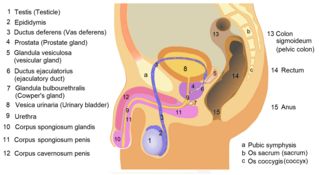
The male reproductive system consists of a number of sex organs that play a role in the process of human reproduction. These organs are located on the outside of the body, and within the pelvis.

The human reproductive system includes the male reproductive system, which functions to produce and deposit sperm, and the female reproductive system, which functions to produce egg cells and to protect and nourish the fetus until birth. Humans have a high level of sexual differentiation. In addition to differences in nearly every reproductive organ, there are numerous differences in typical secondary sex characteristics.
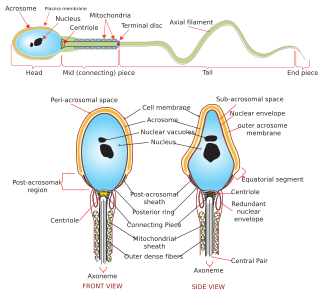
Sperm is the male reproductive cell, or gamete, in anisogamous forms of sexual reproduction. Animals produce motile sperm with a tail known as a flagellum, which are known as spermatozoa, while some red algae and fungi produce non-motile sperm cells, known as spermatia. Flowering plants contain non-motile sperm inside pollen, while some more basal plants like ferns and some gymnosperms have motile sperm.
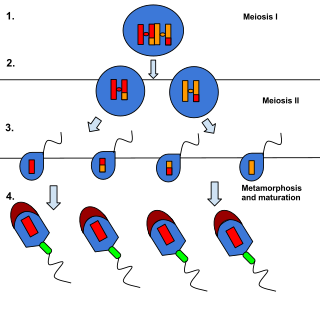
Spermiogenesis is the final stage of spermatogenesis, during which the spermatids develop into mature spermatozoa. At the beginning of the stage, the spermatid is a more or less circular cell containing a nucleus, Golgi apparatus, centriole and mitochondria; by the end of the process, it has radically transformed into an elongated spermatozoon, complete with a head, midpiece, and tail.
The blood–testis barrier is a physical barrier between the blood vessels and the seminiferous tubules of the animal testes. The name "blood-testis barrier" is misleading as it is not a blood-organ barrier in a strict sense, but is formed between Sertoli cells of the seminiferous tubule and isolates the further developed stages of germ cells from the blood. A more correct term is the Sertoli cell barrier (SCB).
Spermatogenesis arrest is known as the interruption of germinal cells of specific cellular type, which elicits an altered spermatozoa formation. Spermatogenic arrest is usually due to genetic factors resulting in irreversible azoospermia. However some cases may be consecutive to hormonal, thermic, or toxic factors and may be reversible either spontaneously or after a specific treatment. Spermatogenic arrest results in either oligospermia or azoospermia in men. It is quite a difficult condition to proactively diagnose as it tends to affect those who have normal testicular volumes; a diagnosis can be made however through a testicular biopsy.
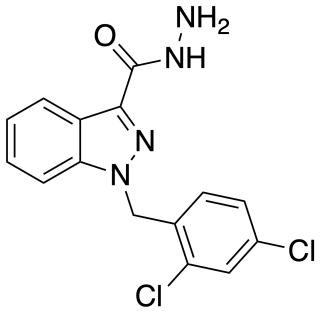
Adjudin (AF-2364) is a drug which is under development as a potential non-hormonal male contraceptive drug, which acts by blocking the production of sperm in the testes, but without affecting testosterone production. It is an analogue of the chemotherapy drug lonidamine, an indazole-carboxylic acid, and further studies continue to be conducted into this family of drugs as possible contraceptives.
Sertoli cell-only syndrome (SCOS), also known as germ cell aplasia, is defined by azoospermia where the testicular seminiferous tubules are lined solely with sertoli cells. Sertoli cells contribute to the formation of the blood-testis barrier and aid in sperm generation. These cells respond to follicle-stimulating hormone, which is secreted by the hypothalamus and aids in spermatogenesis.
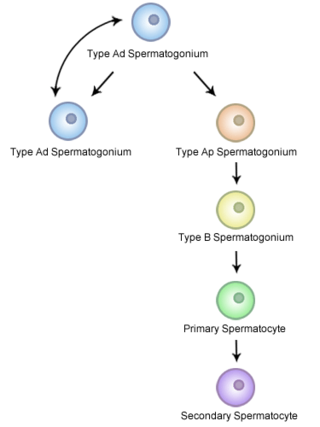
A spermatogonial stem cell (SSC), also known as a type A spermatogonium, is a spermatogonium that does not differentiate into a spermatocyte, a precursor of sperm cells. Instead, they continue dividing into other spermatogonia or remain dormant to maintain a reserve of spermatogonia. Type B spermatogonia, on the other hand, differentiate into spermatocytes, which in turn undergo meiosis to eventually form mature sperm cells.
In vitro spermatogenesis is the process of creating male gametes (spermatozoa) outside of the body in a culture system. The process could be useful for fertility preservation, infertility treatment and may further develop the understanding of spermatogenesis at the cellular and molecular level.






