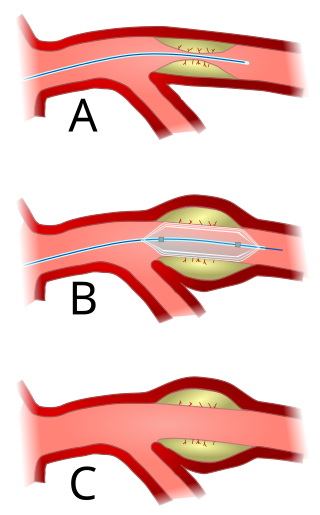
Angioplasty, also known as balloon angioplasty and percutaneous transluminal angioplasty (PTA), is a minimally invasive endovascular procedure used to widen narrowed or obstructed arteries or veins, typically to treat arterial atherosclerosis.

Coronary artery bypass surgery, also known as coronary artery bypass graft, is a surgical procedure to treat coronary artery disease (CAD), the buildup of plaques in the arteries of the heart. It can relieve chest pain caused by CAD, slow the progression of CAD, and increase life expectancy. It aims to bypass narrowings in heart arteries by using arteries or veins harvested from other parts of the body, thus restoring adequate blood supply to the previously ischemic heart.

In medicine, a stent is a tube usually constructed of a metallic alloy or a polymer. It is inserted into the lumen of an anatomic vessel or duct to keep the passageway open. Stenting refers to the placement of a stent. The word "stent" is also used as a verb to describe the placement of such a device, particularly when a disease such as atherosclerosis has pathologically narrowed a structure such as an artery.

Angiography or arteriography is a medical imaging technique used to visualize the inside, or lumen, of blood vessels and organs of the body, with particular interest in the arteries, veins, and the heart chambers. Modern angiography is performed by injecting a radio-opaque contrast agent into the blood vessel and imaging using X-ray based techniques such as fluoroscopy.

A coronary catheterization is a minimally invasive procedure to access the coronary circulation and blood filled chambers of the heart using a catheter. It is performed for both diagnostic and interventional (treatment) purposes.

Stenosis is the abnormal narrowing of a blood vessel or other tubular organ or structure such as foramina and canals. It is also sometimes called a stricture.
Intravascular ultrasound (IVUS) or intravascular echocardiography is a medical imaging methodology using a specially designed catheter with a miniaturized ultrasound probe attached to the distal end of the catheter. The proximal end of the catheter is attached to computerized ultrasound equipment. It allows the application of ultrasound technology, such as piezoelectric transducer or CMUT, to see from inside blood vessels out through the surrounding blood column, visualizing the endothelium of blood vessels.

Cardiac catheterization is the insertion of a catheter into a chamber or vessel of the heart. This is done both for diagnostic and interventional purposes.

Percutaneous coronary intervention (PCI) is a minimally invasive non-surgical procedure used to treat narrowing of the coronary arteries of the heart found in coronary artery disease. The procedure is used to place and deploy coronary stents, a permanent wire-meshed tube, to open narrowed coronary arteries. PCI is considered 'non-surgical' as it uses a small hole in a peripheral artery (leg/arm) to gain access to the arterial system, an equivalent surgical procedure would involve the opening of the chest wall to gain access to the heart area. The term 'coronary angioplasty with stent' is synonymous with PCI. The procedure visualises the blood vessels via fluoroscopic imaging and contrast dyes. PCI is performed by an interventional cardiologists in a catheterization laboratory setting.
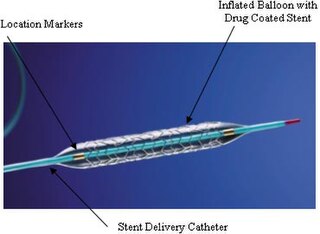
A drug-eluting stent (DES) is a tube made of a mesh-like material used to treat narrowed arteries in medical procedures both mechanically and pharmacologically. A DES is inserted into a narrowed artery using a delivery catheter usually inserted through a larger artery in the groin or wrist. The stent assembly has the DES mechanism attached towards the front of the stent, and usually is composed of the collapsed stent over a collapsed polymeric balloon mechanism, the balloon mechanism is inflated and used to expand the meshed stent once in position. The stent expands, embedding into the occluded artery wall, keeping the artery open, thereby improving blood flow. The mesh design allows for stent expansion and also for new healthy vessel endothelial cells to grow through and around it, securing it in place.
The history of invasive and interventional cardiology is complex, with multiple groups working independently on similar technologies. Invasive and interventional cardiology is currently closely associated with cardiologists, though the development and most of its early research and procedures were performed by diagnostic and interventional radiologists.
Fractional flow reserve (FFR) is a diagnostic technique used in coronary catheterization. FFR measures pressure differences across a coronary artery stenosis to determine the likelihood that the stenosis impedes oxygen delivery to the heart muscle.
A coronary stent is a tube-shaped device placed in the coronary arteries that supply blood to the heart, to keep the arteries open in patients suffering from coronary heart disease. The vast majority of stents used in modern interventional cardiology are drug-eluting stents (DES). They are used in a medical procedure called percutaneous coronary intervention (PCI). Coronary stents are divided into two broad types: drug-eluting and bare metal stents. As of 2023, drug-eluting stents were used in more than 90% of all PCI procedures. Stents reduce angina and have been shown to improve survival and decrease adverse events after a patient has suffered a heart attack—medically termed an acute myocardial infarction.

Zotarolimus is an immunosuppressant. It is a semi-synthetic derivative of sirolimus (rapamycin). It was designed for use in stents with phosphorylcholine as a carrier. Zotarolimus, or ABT-578, was originally used on Abbott's coronary stent platforms to reduce early inflammation and restenosis; however, Zotarolimus failed Abbott's primary endpoint to bring their stent/drug delivery system to market. The drug was sold/distributed to Medtronic for use on their stent platforms, which is the same drug they use today. Coronary stents reduce early complications and improve late clinical outcomes in patients needing interventional cardiology. The first human coronary stent implantation was first performed in 1986 by Puel et al. However, there are complications associated with stent use, development of thrombosis which impedes the efficiency of coronary stents, haemorrhagic and restenosis complications are problems associated with stents.

Pulmonary artery stenosis (PAS) is a narrowing of the pulmonary artery. The pulmonary artery is a blood vessel moving blood from the right side of the heart to the lungs. This narrowing can be due to many causes, including infection during pregnancy, a congenital heart defect, a problem with blood clotting in childhood or early adulthood, or a genetic change.
Julio Palmaz is a doctor of vascular radiology at University of Texas Health Science Center at San Antonio. He studied at the National University of La Plata in Argentina, earning his medical degree in 1971. He then practiced vascular radiology at the San Martin University Hospital in La Plata before moving to the University of Texas Health and Science Center at San Antonio. He is known for inventing the balloon-expandable stent, for which he received a patent filed in 1985. It was recognized in Intellectual Property International Magazine as one of "Ten Patents that Changed the World" in the last century. His early stent research artifacts are now part of the medical collection of the Smithsonian Institution in Washington, DC. He continues to innovate on his initial designs, developing new endovascular devices.

A bioresorbable stent is a tube-like device (stent) that is used to open and widen clogged heart arteries and then dissolves or is absorbed by the body. It is made from a material that can release a drug to prevent scar tissue growth. It can also restore normal vessel function and avoid long-term complications of metal stents.
Neointimal hyperplasia refers to proliferation and migration of vascular smooth muscle cells primarily in the tunica intima, resulting in the thickening of arterial walls and decreased arterial lumen space. Neointimal hyperplasia is the major cause of restenosis after percutaneous coronary interventions such as stenting or angioplasty. The term neointima is used because the cells in the hyperplastic regions of the vascular wall have histological characteristics of both intima and normal artery cells.
A dual therapy stent is a coronary artery stent that combines the technology of an antibody-coated stent and a drug-eluting stent. Currently, second-generation drug-eluting stents require long-term use of dual-antiplatelet therapy, which increases the risk of major bleeding occurrences in patients. Compared to drug-eluting stents, dual therapy stents have improved vessel regeneration and cell proliferation capabilities. As a result, dual therapy stents were developed to reduce the long-term need for dual-antiplatelet therapy.
Alfredo E. Rodríguez is an Argentine interventional cardiologist, clinical researcher, and author. He is the Chief of Interventional Cardiology Service at Otamendi Hospital and Director and Founder of the Cardiovascular Research Center (CECI) a non -profit Research Organization in Buenos Aires Argentina.

