Nasal nitric oxide levels, light microscopy of biopsies for ciliary beat pattern and frequency, and electron microscopic examination of dynein arms.[5]
Respiratory epithelialmotile cilia, which resemble microscopic "hairs" (although structurally and biologically unrelated to hair), are complex organelles that beat synchronously in the respiratory tract, moving mucus toward the throat. Normally, cilia beat 7 to 22 times per second, and any impairment can result in poor mucociliary clearance, with subsequent upper and lower respiratory infection. Cilia also are involved in other biological processes (such as nitric oxide production), currently the subject of dozens of research efforts.[7]
Signs and symptoms
Sagittal CT image showing "tree in bud" appearance of mucous impaction in distal small airways related to primary ciliary dyskinesiaCT image showing dilated and thickened medium-sized airways (bronchiectasis) in a patient with Kartagener syndromeOblique sagittal CT image showing lower lobe cylindrical bronchiectasis in the same patient
Around 80% of people with primary ciliary dyskinesia experience respiratory problems beginning within a day of birth. Many have a collapsed lobe of the lung and blood oxygen low enough to require treatment with supplemental oxygen.[1] Within the first few months of life, most develop a chronic mucus-producing cough and runny nose.[1] The main consequence of impaired ciliary function is reduced or absent mucus clearance from the lungs, and susceptibility to chronic recurrent respiratory infections, including sinusitis, bronchitis, pneumonia, and otitis media. Progressive damage to the respiratory system is common, including progressive bronchiectasis beginning in early childhood, and sinus disease (sometimes becoming severe in adults). However, diagnosis is often missed early in life despite the characteristic signs and symptoms.[2] In males, immotility of sperm can lead to infertility, although conception remains possible through the use of in vitro fertilization, there also are reported cases where sperm were able to move.[8] Trials have also shown that there is a marked reduction in fertility in females with Kartagener's syndrome due to dysfunction of the oviductal cilia.[9]
Many affected individuals experience hearing loss and show symptoms of otitis media which demonstrates variable responsiveness to the insertion of myringotomy tubes or grommets. Some patients have a poor sense of smell, which is believed to accompany high mucus production in the sinuses (although others report normal– or even acute– sensitivity to smell and taste). Clinical progression of the disease is variable, with lung transplantation required in severe cases. Susceptibility to infections can be drastically reduced by an early diagnosis. Treatment with various chest physiotherapy techniques has been observed to reduce the incidence of lung infection and to slow the progression of bronchiectasis dramatically. Aggressive treatment of sinus disease beginning at an early age is believed to slow long-term sinus damage (although this has not yet been adequately documented). Aggressive measures to enhance clearance of mucus, prevent respiratory infections, and treat bacterial superinfections have been observed to slow lung-disease progression. The predicted incidence is 1 in approximately 7500.[10]
Genetics
PCD is a genetically heterogeneous disorder affecting motile cilia[4] which are made up of approximately 250 proteins.[11] Around 90%[12] of individuals with PCD have ultrastructural defects affecting protein(s) in the outer and/or inner dynein arms, which give cilia their motility, with roughly 38%[12] of these defects caused by mutations on two genes, DNAI1 and DNAH5, both of which code for proteins found in the ciliary outer dynein arm.[13]
There is an international effort to identify genes that code for inner dynein arm proteins or proteins from other ciliary structures (radial spokes, central apparatus, etc.) associated with PCD.[6] The role of DNAH5 in heterotaxy syndromes and left-right asymmetry is also under investigation. At least 50 genes have been implicated in this condition.[10]
Another gene associated with this condition is GAS2L2.[14]
Pathophysiology
CT image showing situs inversus. The liver is normally on the right side of the body and the spleen on the left, they are switched in this patient with situs inversus.
This condition is genetically inherited. Structures that make up the cilia, including inner and/or outer dynein arms, central apparatus, radial spokes, etc. are missing or dysfunctional and thus the axoneme structure lacks the ability to move. Axonemes are the elongated structures that make up cilia and flagella. Additionally, there may be chemical defects that interfere with ciliary function in the presence of adequate structure. Whatever the underlying cause, dysfunction of the cilia begins during and impacts the embryologic phase of development.[6]
Axial CT image showing dextrocardia with the IVC and morphologic right ventricle on the left and the left ventricle on the right
Specialised monocilia known as nodal cilia are at the heart of this problem. They lack the central-pair microtubules of ordinary motile cilia and so rotate clockwise rather than beat; in the primitive node at the anterior end of the primitive streak in the embryo, these are angled posteriorly[15][16] such that they describe a D-shape rather than a circle.[16] This has been shown to generate a net leftward flow in mouse and chick embryos, and sweeps the protein to the left, triggering normal asymmetrical development.[17]
However, in some individuals with PCD, mutations thought to be in the gene coding for the key structural protein left-right dynein (lrd)[4] result in monocilia which do not rotate. There is therefore no flow generated in the node, Shh moves at random within it, and 50% of those affected develop situs inversus, which can occur with or without dextrocardia, where the laterality of the internal organs is the mirror-image of normal. Affected individuals therefore have Kartagener syndrome. This is not the case with some PCD-related genetic mutations: at least 6% of the PCD population have a condition called situs ambiguus or heterotaxy, where organ placement or development is neither typical (situs solitus) nor totally reversed (situs inversus totalis) but is a hybrid of the two.[6] Splenic abnormalities such as polysplenia, asplenia and complex congenital heart defects are more common in individuals with situs ambiguus and PCD, as they are in all individuals with situs ambiguus.[18]
The genetic forces linking failure of nodal cilia and situs issues and the relationship of those forces to PCD are the subject of intense research interest. However, knowledge in this area is constantly advancing.[citation needed]
Diagnosis
Several diagnostic tests for this condition have been proposed.[5] These include nasal nitric oxide levels as a screening test, light microscopy of biopsies for ciliary beat pattern and frequency and electron microscopic examination of dynein arms, as the definite diagnosis method. Genetic testing has also been proposed but this is difficult given that there are multiple genes involved.[6]
Classification
Axial CT image showing chronic sinusitis in an individual with Kartagener syndrome
When accompanied by the combination of situs inversus (reversal of the internal organs), chronic sinusitis, and bronchiectasis, it is known as Kartagener syndrome[3] (only 50% of primary ciliary dyskinesia cases include situs inversus).[11]
Treatment
There are no standardized effective treatment strategies for the condition. Current therapies for PCD are extrapolated from Cystic Fibrosis and patients with non-CF bronchiectasis and lack validation for PCD-specific use.[19]
Severe fatal respiratory failure can develop; long-term treatment with macrolides such as clarithromycin, erythromycin and azithromycin has been empirically applied for the treatment of primary ciliary dyskinesia in Japan, though controversial due to the effects of the medications.[20]
Prognosis
There is no reliable estimate of life expectancy for people with PCD.[21] However, there is evidence that PCD, is a life altering[22] life shortening[23] multi-system condition, with some people progressing to lung transplant.[24][25][26][27]
Decline in lung function in people with PCD has been observed in most studies,[28][25][29][30][31] with FEV1 decline causing deterioration in health, impacting on, and reducing quality of life.[32] With such a genetically and phenotypically heterogenous group, observation of median/mean decline in lung function risks regression to the mean, missing those groups with significantly worse lung function,[10][33][34][35][36][37][38] masked by those with milder phenotypes.[10][36]
The recent body of published data from respected clinicians in (the United Kingdom, Europe, North America, Canada and Israel) indicate that PCD morbidity and mortality appear to have been under-estimated by the medical community.[28][25][39][40][41] While prospective outcome data is limited due to the early-stage patient registries, there is a growing body of evidence[25][39][40][41][42] that dispels any "myth that PCD is a mild disease.[25][39][40][41][43][44][45]
The studies presented here demonstrate that children with PCD typically have worse lung function than those with cystic fibrosis.[28][31][29][46][30] While previously it was thought that with early diagnosis, lung function could largely be prevented in children with PCD,[47] it is key to note that poor lung function is repeatedly observed in children with PCD[46][28][31][29]1,30,32,33,36–38 and some develop bronchiectasis during[48][33] childhood.
Research
Research to further the understanding of cilia, with the future aims of functional restoration of motile cilia is advancing. However, charitable funding for medical research, particularly for rare disease is vital and in the UK contributes to more than 50% of grants. The UK registered charity PCD Research supports research into PCD worldwide, with the ultimate aim of funding potentially curative research.[7] Future promising avenues for functional replacement of cilia involve antisense, gene editing via CRISPR-Cas9 and mRNA therapies. At present there have only been a handful of interventional trials in PCD.[49]
History
The classic symptom combination associated with PCD was first described in 1904 by A. K. Siewert,[50] while Manes Kartagener published his first report on the subject in 1933.[51] The disorder is rarely referred to as Siewert's syndrome or Siewert-Kartagener syndrome.[52]
Related Research Articles
The cilium is a short hair-like membrane protrusion from many types of eukaryotic cell. The cilium has the shape of a slender threadlike projection that extends from the surface of the much larger cell body. Eukaryotic flagella found on sperm cells and many protozoans have a similar structure to motile cilia that enables swimming through liquids; they are longer than cilia and have a different undulating motion.
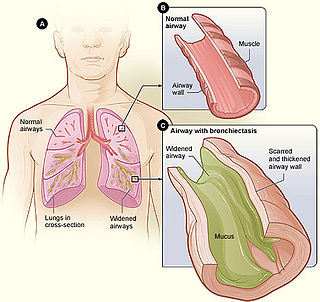
Bronchiectasis is a disease in which there is permanent enlargement of parts of the airways of the lung. Symptoms typically include a chronic cough with mucus production. Other symptoms include shortness of breath, coughing up blood, and chest pain. Wheezing and nail clubbing may also occur. Those with the disease often get lung infections.
Situs inversus is a congenital condition in which the major visceral organs are reversed or mirrored from their normal positions. The normal arrangement of internal organs is known as situs solitus. Although cardiac problems are more common, many people with situs inversus have no medical symptoms or complications resulting from the condition, and until the advent of modern medicine, it was usually undiagnosed.
Respiratory diseases, or lung diseases, are pathological conditions affecting the organs and tissues that make gas exchange difficult in air-breathing animals. They include conditions of the respiratory tract including the trachea, bronchi, bronchioles, alveoli, pleurae, pleural cavity, the nerves and muscles of respiration. Respiratory diseases range from mild and self-limiting, such as the common cold, influenza, and pharyngitis to life-threatening diseases such as bacterial pneumonia, pulmonary embolism, tuberculosis, acute asthma, lung cancer, and severe acute respiratory syndromes, such as COVID-19. Respiratory diseases can be classified in many different ways, including by the organ or tissue involved, by the type and pattern of associated signs and symptoms, or by the cause of the disease.
Nephronophthisis is a genetic disorder of the kidneys which affects children. It is classified as a medullary cystic kidney disease. The disorder is inherited in an autosomal recessive fashion and, although rare, is the most common genetic cause of childhood kidney failure. It is a form of ciliopathy. Its incidence has been estimated to be 0.9 cases per million people in the United States, and 1 in 50,000 births in Canada.
Dynein axonemal heavy chain 5 is a protein that in humans is encoded by the DNAH5 gene.
Dynein heavy chain 9, axonemal is a protein that in humans is encoded by the DNAH9 gene.
Dynein axonemal intermediate chain 1 is a protein that in humans is encoded by the DNAI1 gene.
Mucociliary clearance (MCC), mucociliary transport, or the mucociliary escalator describes the self-clearing mechanism of the airways in the respiratory system. It is one of the two protective processes for the lungs in removing inhaled particles including pathogens before they can reach the delicate tissue of the lungs. The other clearance mechanism is provided by the cough reflex. Mucociliary clearance has a major role in pulmonary hygiene.
Renal–hepatic–pancreatic dysplasia is an autosomal recessive congenital disorder characterized by pancreatic fibrosis, renal dysplasia and hepatic dysgenesis. An association with NPHP3 has been described. It was characterized in 1959.
A ciliopathy is any genetic disorder that affects the cellular cilia or the cilia anchoring structures, the basal bodies, or ciliary function. Primary cilia are important in guiding the process of development, so abnormal ciliary function while an embryo is developing can lead to a set of malformations that can occur regardless of the particular genetic problem. The similarity of the clinical features of these developmental disorders means that they form a recognizable cluster of syndromes, loosely attributed to abnormal ciliary function and hence called ciliopathies. Regardless of the actual genetic cause, it is clustering of a set of characteristic physiological features which define whether a syndrome is a ciliopathy.
The transmission electron microscope (TEM) is used as an important diagnostic tool to screen human tissues at high magnification and at high resolution, often in conjunction with other methods, particularly light microscopy and immunofluorescence techniques. The TEM was first used extensively for this purpose in the 1980s, especially for identifying the markers of cell differentiation to identify tumours, and in renal disease. Immunolabelling techniques are now generally used instead of the TEM for tumour diagnosis but the technique retains a critical role in the diagnosis of renal disease and a range of other conditions. One example is Primary ciliary dyskinesia (PCD), a rare ciliopathy which affects the action of cilia. TEM images of ciliary axonemes are examined using TEM and abnormalities of structure can provide a positive diagnosis in some cases.
Dynein axonemal intermediate chain 2 also known as axonemal dynein intermediate chain 2, is a protein that in humans is encoded by the DNAI2 gene.
Dynein axonemal light chain 1, (LC1) is a protein that in humans is encoded by the DNAL1 gene.
Sensenbrenner syndrome is a rare multisystem disease first described by Judith A. Sensenbrenner in 1975. It is inherited in an autosomal recessive fashion, and a number of genes appear to be responsible. Three genes responsible have been identified: intraflagellar transport (IFT)122 (WDR10), IFT43—a subunit of the IFT complex A machinery of primary cilia, and WDR35
CCDC40 is the gene in humans that encodes the protein named coiled-coil domain containing 40.
Pleasantine Mill is a cell biologist and group leader at the MRC Human Genetics Unit at the University of Edinburgh. She won the 2018 British Society for Cell Biology Women in Cell Biology Early Career Medal.
Alfons Karlovich Siewert (1872–1922), also called Alfons Karlovich Zivert or Alfonse-Ferdinand-Julius-Zivert, was a Ukrainian physician, who hailed from a German family closely allied to the Tsar and Imperial Russia. He is known for his eponymous contribution to the Siewert-Kartagener syndrome.
Manes Kartagener was a Swiss internist of Polish-Jewish origins.
1 2 Coren, M. E; Meeks, M; Morrison, I; Buchdahl, R. M; Bush, A (2002). "Primary ciliary dyskinesia: Age at diagnosis and symptom history". Acta Paediatrica. 91 (6): 667–9. doi:10.1080/080352502760069089. PMID12162599.
1 2 Zariwala, Maimoona A; Knowles, Michael R; Leigh, Margaret W (December 5, 2019). "Primary Ciliary Dyskinesia". University of Washington, Seattle. PMID20301301. Retrieved October 16, 2023.
↑ Bustamante-Marin, Ximena M.; Yin, Wei-Ning; Sears, Patrick R.; Werner, Michael E.; Brotslaw, Eva J.; Mitchell, Brian J.; Jania, Corey M.; Zeman, Kirby L.; Rogers, Troy D.; Herring, Laura E.; Refabért, Luc; Thomas, Lucie; Amselem, Serge; Escudier, Estelle; Legendre, Marie; Grubb, Barbara R.; Knowles, Michael R.; Zariwala, Maimoona A.; Ostrowski, Lawrence E. (2019). "Lack of GAS2L2 Causes PCD by Impairing Cilia Orientation and Mucociliary Clearance". The American Journal of Human Genetics. 104 (2): 229–245. doi:10.1016/j.ajhg.2018.12.009. PMC6372263. PMID30665704.
↑ Kartagener, M. (September 1933). "Zur Pathogenese der Bronchiektasien" [On the pathogenesis of bronchiectasis]. Beiträge zur Klinik der Tuberkulose und spezifischen Tuberkulose-Forschung (in German). 83 (4): 489–501. doi:10.1007/BF02141468. S2CID7708592.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.