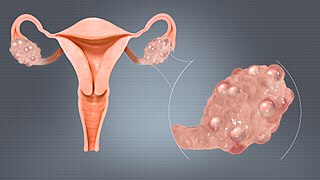
Polycystic ovary syndrome, or polycystic ovarian syndrome (PCOS), is the most common endocrine disorder in women of reproductive age. The syndrome is named after cysts which form on the ovaries of some people with this condition, though this is not a universal symptom, and not the underlying cause of the disorder.

Acne, also known as acne vulgaris, is a long-term skin condition that occurs when dead skin cells and oil from the skin clog hair follicles. Typical features of the condition include blackheads or whiteheads, pimples, oily skin, and possible scarring. It primarily affects skin with a relatively high number of oil glands, including the face, upper part of the chest, and back. The resulting appearance can lead to lack of confidence, anxiety, reduced self-esteem, and, in extreme cases, depression or thoughts of suicide.

Hirsutism is excessive body hair on parts of the body where hair is normally absent or minimal. The word is from early 17th century: from Latin hirsutus meaning "hairy". It usually refers to a male pattern of hair growth in a female that may be a sign of a more serious medical condition, especially if it develops well after puberty. Cultural stigma against hirsutism can cause much psychological distress and social difficulty. Discrimination based on facial hirsutism often leads to the avoidance of social situations and to symptoms of anxiety and depression.

Electrology is the practice of electrical hair removal to permanently remove human hair from the body. Electrolysis is the actual process of removing hair using electricity.

Hair removal, also known as epilation or depilation, is the deliberate removal of body hair or head hair.
Intense pulsed light (IPL) is a technology used by cosmetic and medical practitioners to perform various skin treatments for aesthetic and therapeutic purposes, including hair removal, photorejuvenation as well as to alleviate dermatologic diseases such as acne. IPL is increasingly used in optometry and ophthalmology as well, to treat evaporative dry eye disease due to meibomian gland dysfunction.

Laser hair removal is the process of hair removal by means of exposure to pulses of laser light that destroy the hair follicle. It had been performed experimentally for about twenty years before becoming commercially available in 1995 and 1996. One of the first published articles describing laser hair removal was authored by the group at Massachusetts General Hospital in 1998. Laser hair removal is widely practiced in clinics, and even in homes using devices designed and priced for consumer self-treatment. Many reviews of laser hair removal methods, safety, and efficacy have been published in the dermatology literature.
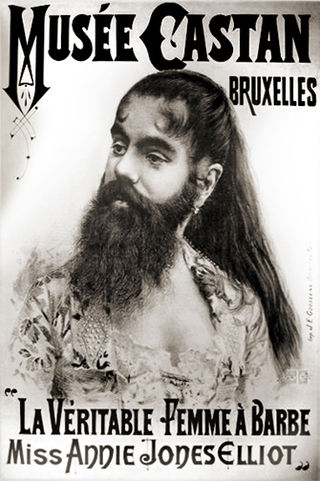
A bearded lady is a woman with a naturally occurring beard normally due to the condition known as hirsutism or hypertrichosis. Hypertrichosis causes people of either sex to develop excess hair over their entire body, while hirsutism is restricted to females and only causes excessive hair growth in the nine body areas mentioned by Ferriman and Gallwey.

Keratosis pilaris is a common, autosomal-dominant, genetic condition of the skin's hair follicles characterized by the appearance of possibly itchy, small, gooseflesh-like bumps, with varying degrees of reddening or inflammation. It most often appears on the outer sides of the upper arms, thighs, face, back, and buttocks; KP can also occur on the hands, and tops of legs, sides, or any body part except glabrous (hairless) skin. Often the lesions can appear on the face, which may be mistaken for acne or folliculitis.
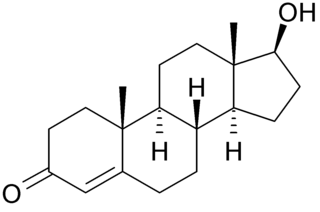
Hyperandrogenism is a medical condition characterized by high levels of androgens. It is more common in women than men. Symptoms of hyperandrogenism may include acne, seborrhea, hair loss on the scalp, increased body or facial hair, and infrequent or absent menstruation. Complications may include high blood cholesterol and diabetes. It occurs in approximately 5% of women of reproductive age.

Hypertrichosis is an abnormal amount of hair growth over the body. The two distinct types of hypertrichosis are generalized hypertrichosis, which occurs over the entire body, and localized hypertrichosis, which is restricted to a certain area. Hypertrichosis can be either congenital or acquired later in life. The excess growth of hair occurs in areas of the skin with the exception of androgen-dependent hair of the pubic area, face, and axillary regions.
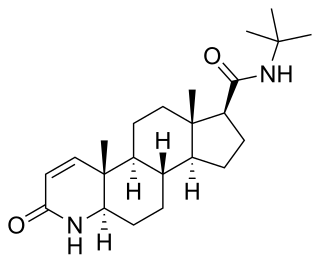
Finasteride, sold under the brand names Proscar and Propecia among others, is a medication used to treat pattern hair loss and benign prostatic hyperplasia (BPH) in men. It can also be used to treat excessive hair growth in women. It is usually taken orally but there are topical formulations for patients with hair loss, designed to minimize systemic exposure by acting specifically on hair follicles.

Vellus hair is short, thin, light-colored, and barely noticeable hair that develops on most of a human’s body during childhood. Exceptions include the lips, the back of the ear, the palm of the hand, the sole of the foot, some external genital areas, the navel, and scar tissue. The density of hair – the number of hair follicles per area of skin – varies from person to person. Each strand of vellus hair is usually less than 2 mm long and the follicle is not connected to a sebaceous gland.

Pseudofolliculitis barbae (PFB) is a type of irritant folliculitis that commonly affects men who have curly or coarse facial hair. It occurs when hair curls back into the skin after shaving, causing inflammation, redness, and bumps. This can lead to ingrown hairs, scarring, and skin discoloration. PFB can be treated with various methods, including changing shaving habits, using topical creams or ointments, and undergoing laser hair removal. Prevention measures include proper shaving techniques, using sharp razors, and avoiding too close a shave.
The management of hair loss, includes prevention and treatment of alopecia, baldness, and hair thinning, and regrowth of hair.

A comedo is a clogged hair follicle (pore) in the skin. Keratin combines with oil to block the follicle. A comedo can be open (blackhead) or closed by skin (whitehead) and occur with or without acne. The word "comedo" comes from the Latin comedere, meaning "to eat up", and was historically used to describe parasitic worms; in modern medical terminology, it is used to suggest the worm-like appearance of the expressed material.
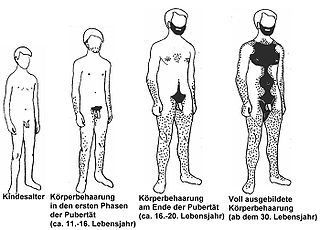
Body hair, or androgenic hair, is terminal hair that develops on the human body during and after puberty. It is different from head hair and also from less visible vellus hair, which is much finer and lighter in colour. Growth of androgenic hair is related to the level of androgens and the density of androgen receptors in the dermal papillae. Both must reach a threshold for the proliferation of hair follicle cells.

Pattern hair loss (also known as androgenetic alopecia (AGA)) is a hair loss condition that primarily affects the top and front of the scalp. In male-pattern hair loss (MPHL), the hair loss typically presents itself as either a receding front hairline, loss of hair on the crown (vertex) of the scalp, or a combination of both. Female-pattern hair loss (FPHL) typically presents as a diffuse thinning of the hair across the entire scalp.

Supernumerary nipples–uropathies–Becker's nevus syndrome is a skin condition that may be associated with genitourinary tract abnormalities. Supernumerary nipples, also referred to as polythelia or accessory nipples, is a pigmented lesion of the skin that is present at birth. This pigmentation usually occurs along the milk lines, which are the precursors to breast and nipple development. Clinically, this congenital condition is generally considered benign, but some studies have suggested there may be an association with kidney diseases and cancers of the urogenital system.

The HAIR-AN syndrome is a rare subtype of polycystic ovary syndrome (PCOS) characterized by hyperandrogenism (HA), insulin resistance (IR) and acanthosis nigricans (AN). The symptoms of the HAIR-AN syndrome are largely due to severe insulin resistance, which can be secondary to blocking antibodies against the insulin receptor or genetically absent/reduced insulin receptor number/function. Insulin resistance leads to hyperinsulinemia which, in turn, leads to an excess production of androgen hormones by the ovaries. High levels of androgen hormones (hyperandrogenism) in females causes excessive hair growth, acne and irregular menstruation. Patients with both underlying mechanisms of insulin resistance may have more severe hyperandrogenism. Insulin resistance is also associated with diabetes, heart disease and excessive darkening of the skin
