
Arthritis is a term often used to mean any disorder that affects joints. Symptoms generally include joint pain and stiffness. Other symptoms may include redness, warmth, swelling, and decreased range of motion of the affected joints. In some types of arthritis, other organs are also affected. Onset can be gradual or sudden.

Giant cell arteritis (GCA), also called temporal arteritis, is an inflammatory autoimmune disease of large blood vessels. Symptoms may include headache, pain over the temples, flu-like symptoms, double vision, and difficulty opening the mouth. Complications can include blockage of the artery to the eye with resulting blindness, as well as aortic dissection, and aortic aneurysm. GCA is frequently associated with polymyalgia rheumatica. It can be confirmed by biopsy of the temporal artery in about 90% of people.
Rheumatology is a branch of medicine devoted to the diagnosis and management of disorders whose common feature is inflammation in the bones, muscles, joints, and internal organs. Rheumatology covers more than 100 different complex diseases, collectively known as rheumatic diseases, which includes many forms of arthritis as well as lupus and Sjögren's syndrome. Doctors who have undergone formal training in rheumatology are called rheumatologists.
The erythrocyte sedimentation rate is the rate at which red blood cells in anticoagulated whole blood descend in a standardized tube over a period of one hour. It is a common hematology test, and is a non-specific measure of inflammation. To perform the test, anticoagulated blood is traditionally placed in an upright tube, known as a Westergren tube, and the distance which the red blood cells fall is measured and reported in millimetres at the end of one hour.

Fifth disease, also known as erythema infectiosum and slapped cheek syndrome, is a common and contagious disease caused by infection with parvovirus B19. This virus was discovered in 1975 and can cause other diseases besides fifth disease. Fifth disease typically presents as a rash and is most common in children. While parvovirus B19 can affect people of all ages, only two out of ten individuals will present with symptoms.

Ankylosing spondylitis (AS) is a type of arthritis from the disease spectrum of axial spondyloarthritis. It is characterized by long-term inflammation of the joints of the spine, typically where the spine joins the pelvis. With AS, eye and bowel problems—as well as back pain—may occur. Joint mobility in the affected areas sometimes worsens over time. Ankylosing spondylitis is believed to involve a combination of genetic and environmental factors. More than 90% of people affected in the UK have a specific human leukocyte antigen known as the HLA-B27 antigen. The underlying mechanism is believed to be autoimmune or autoinflammatory. Diagnosis is based on symptoms with support from medical imaging and blood tests. AS is a type of seronegative spondyloarthropathy, meaning that tests show no presence of rheumatoid factor (RF) antibodies.
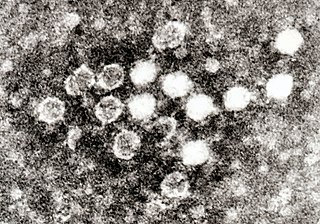
Human parvovirus B19, generally referred to as B19 virus(B19V),parvovirus B19 or sometimes erythrovirus B19, is a known human virus in the family Parvoviridae, genus Erythroparvovirus; it measures only 23–26 nm in diameter. Human parvovirus b19 is a below-species classification of Erythroparvovirus primate1. The name is derived from Latin parvum, meaning small, reflecting the fact that B19 ranks among the smallest DNA viruses. B19 virus is most known for causing disease in the pediatric population; however, it can also affect adults. It is the classic cause of the childhood rash called fifth disease or erythema infectiosum, or "slapped face syndrome". The name comes from it being the fifth in a list of historical classifications of common skin rash illnesses in children.

Vasculitis is a group of disorders that destroy blood vessels by inflammation. Both arteries and veins are affected. Lymphangitis is sometimes considered a type of vasculitis. Vasculitis is primarily caused by leukocyte migration and resultant damage. Although both occur in vasculitis, inflammation of veins (phlebitis) or arteries (arteritis) on their own are separate entities.

Henoch–Schönlein purpura (HSP), also known as IgA vasculitis, is a disease of the skin, mucous membranes, and sometimes other organs that most commonly affects children. In the skin, the disease causes palpable purpura, often with joint pain and abdominal pain. With kidney involvement, there may be a loss of small amounts of blood and protein in the urine, but this usually goes unnoticed; in a small proportion of cases, the kidney involvement proceeds to chronic kidney disease. HSP is often preceded by an infection, such as a throat infection.
Polyarteritis nodosa (PAN) is a systemic necrotizing inflammation of blood vessels (vasculitis) affecting medium-sized muscular arteries, typically involving the arteries of the kidneys and other internal organs but generally sparing the lungs' circulation. Small aneurysms are strung like the beads of a rosary, therefore making this "rosary sign" an important diagnostic feature of the vasculitis. PAN is sometimes associated with infection by the hepatitis B or hepatitis C virus. The condition may be present in infants.
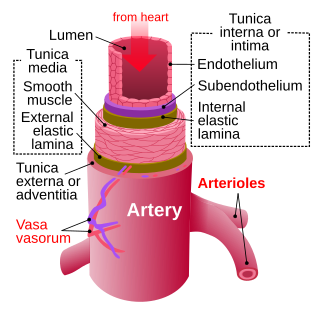
Arteritis is a vascular disorder characterized by inflammation of the walls of arteries, usually as a result of infection or autoimmune responses. Arteritis, a complex disorder, is still not entirely understood. Arteritis may be distinguished by its different types, based on the organ systems affected by the disease. A complication of arteritis is thrombosis, which can be fatal. Arteritis and phlebitis are forms of vasculitis.
Posterior ischemic optic neuropathy (PION) is a medical condition characterized by damage to the retrobulbar portion of the optic nerve due to inadequate blood flow (ischemia) to the optic nerve. Despite the term posterior, this form of damage to the eye's optic nerve due to poor blood flow also includes cases where the cause of inadequate blood flow to the nerve is anterior, as the condition describes a particular mechanism of visual loss as much as the location of damage in the optic nerve. In contrast, anterior ischemic optic neuropathy (AION) is distinguished from PION by the fact that AION occurs spontaneously and on one side in affected individuals with predisposing anatomic or cardiovascular risk factors.

A giant cell is a mass formed by the union of several distinct cells, often forming a granuloma.

Pure red cell aplasia (PRCA) or erythroblastopenia refers to a type of aplastic anemia affecting the precursors to red blood cells but usually not to white blood cells. In PRCA, the bone marrow ceases to produce red blood cells. There are multiple etiologies that can cause PRCA. The condition has been first described by Paul Kaznelson in 1922.
Arteritic anterior ischemic optic neuropathy is vision loss that occurs in giant cell arteritis. Temporal arteritis is an inflammatory disease of medium-sized blood vessels that happens especially with advancing age. AAION occurs in about 15-20 percent of patients with temporal arteritis. Damage to the blood vessels supplying the optic nerves leads to insufficient blood supply (ischemia) to the nerve and subsequent optic nerve fiber death. Most cases of AAION result in nearly complete vision loss first to one eye. If the temporal arteritis is left untreated, the affected eye will likely suffer vision loss as well within 1–2 weeks. Arteritic AION (AAION) falls under the general category of anterior ischemic optic neuropathy (AION), which also includes non-arteritic AION (NAION). AAION is considered an eye emergency, immediate treatment is essential to rescue remaining vision.
A neuromuscular disease is any disease affecting the peripheral nervous system (PNS), the neuromuscular junctions, or skeletal muscles, all of which are components of the motor unit. Damage to any of these structures can cause muscle atrophy and weakness. Issues with sensation can also occur.
Aortitis is the inflammation of the aortic wall. The disorder is potentially life-threatening and rare. It is reported that there are only 1–3 new cases of aortitis per year per million people in the United States and Europe. Aortitis is most common in people 10 to 40 years of age.
Cerebral vasculitis is vasculitis involving the brain and occasionally the spinal cord. It affects all of the vessels: very small blood vessels (capillaries), medium-size blood vessels, or large blood vessels. If blood flow in a vessel with vasculitis is reduced or stopped, the parts of the body that receive blood from that vessel begins to die. It may produce a wide range of neurological symptoms, such as headache, skin rashes, feeling very tired, joint pains, difficulty moving or coordinating part of the body, changes in sensation, and alterations in perception, thought or behavior, as well as the phenomena of a mass lesion in the brain leading to coma and herniation. Some of its signs and symptoms may resemble multiple sclerosis. 10% have associated bleeding in the brain.

Necrotizing vasculitis, also called systemic necrotizing vasculitis, is a general term for the inflammation of veins and arteries that develops into necrosis and narrows the vessels.

Acute visual loss is a rapid loss of the ability to see. It is caused by many ocular conditions like retinal detachment, glaucoma, macular degeneration, and giant cell arteritis, etc.
