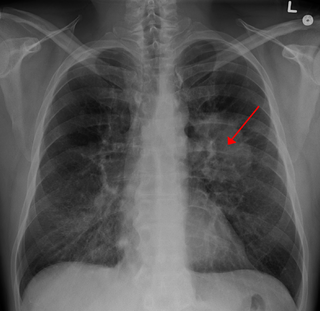
A lung nodule or pulmonary nodule is a relatively small focal density in the lung. A solitary pulmonary nodule (SPN) or coin lesion,[1] is a mass in the lung smaller than three centimeters in diameter. A pulmonary micronodule has a diameter of less than three millimetres.[2] There may also be multiple nodules.
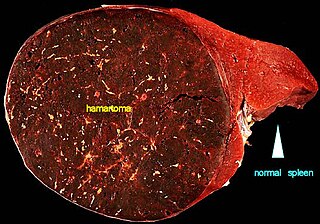
The nodule most commonly represents a benign tumor such as a granuloma or hamartoma, but in around 20% of cases it represents a malignantcancer,[4] especially in older adults and smokers. Conversely, 10 to 20% of patients with lung cancer are diagnosed in this way.[4] If the patient has a history of smoking or the nodule is growing, the possibility of cancer may need to be excluded through further radiological studies and interventions, possibly including surgical resection. The prognosis depends on the underlying condition.
Causes
Not every round spot on a radiological image is a solitary pulmonary nodule: it may be confused with the projection of a structure of the chest wall or skin, such as a nipple, a healing rib fracture or electrocardiographic monitoring.
Size: larger size confers a higher risk of cancer[8]
Location: Upper lobe location is a risk factor for cancer, while a location close to a fissure or the pleura indicates a benign lymph node,[8] especially if having a triangular shape.[9]
Margin morphology: a spiculated margin is a risk factor for cancer.[8] Benign causes tend to have a well defined border, whereas lobulated lesions or those with an irregular margin extending into the neighbouring tissue tend to be malignant.[10] In particular, spiculations are highly predictive of malignancy with a positive predictive value up to 90%.[9] Also, a "notch sign", which is an abrupt indentation of the nodule, increases the risk of cancer, but may also be found in granulomatous diseases.[9]
A triangular perifissural node can be diagnosed as a benign lymph node.[9]
Multiplicity: Where the presence of up to an additional 3 nodules has been found to increase the risk of cancer, but decrease in case of 4 or more additional ones, likely because it indicates a previous granulomatous infection rather than cancer.[8]
Growth rate: solid cancers generally doubles in volume over between 100 and 400 days, while subsolid cancers (generally representing adenocarcinomas) generally doubles in volume over 3 to 5 years.[8] One volume doubling equals approximately a 26% increase in diameter.[8]
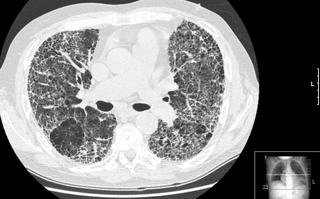
Presence of emphysema and/or fibrosis is a risk factor for cancer.[8] In comparison, the typical size doubling are less than 20 days for infections, and more than 400 days for benign nodules.[11]
Enhancement: If the exam is done as a combined non-contrast and contrast CT, a solitary nodule with an enhancement off less than 15 Hounsfield units (HU), whereas a higher enhancement indicates a malignant tumor (with a sensitivity estimated at 98%).[12]
Areas of fatty tissue (−40 to −120 HU) indicates a hamartoma. However, only about 50% of hamartomas are fat containing.[9]
If there is a central cavity, then a thin wall points to a benign cause whereas a thick wall is associated with malignancy (especially 4mm or less versus 16mm or more).[10]
Low attenuating nodule (in this case a fat containing hamartoma).[9]
Cavitation with relatively thick wall, in this case aspergilloma).[9]
Calcifications and popcorn-like appearance, conferring a diagnosis of hamartoma.
In case of calcifications, a popcorn-like appearance indicates a hamartoma, which is benign.[3]
In case of subsolid nodules, being part solid has a higher risk of cancer than being purely ground glass opacity.
In this case, pleural retraction is seen as a triangular fat component.[9]
Lung nodule abutting a pulmonary cyst.
A lung nodule abutting a pulmonary cyst is a rare finding, yet indicating cancer.[9]
Bubble-like lucencies in the nodule indicate cancer:[9]
Thin slice and maximal intensity projection of a lung nodule, the latter better visualizing vascular convergence.
Vascular convergence is where vessels converge to a nodule without adjoining or contacting the edge of the nodule, and is mainly seen in peripheral subsolid lung cancers.[9] It reflects angiogenesis.[9]
Air bronchograms is defined as a pattern of air-filled bronchi on a background of airless lung, and may be seen in both benign and malignant nodules, but certain patterns thereof may help in risk stratification.[9]
CT densitometry, measuring absolute attenuation on the Hounsfield scale, has low sensitivity and specificity and is not routinely employed, apart from helping to distinguish solid from ground glass lesions, and to confirm visible fatty areas or calcifications.[12]
Nodular density is used to distinguish larger lung tumors, smaller infiltrates or masses with other accompanying characteristics. An often used formal radiological definition is the following: a single lesion in the lung completely surrounded by functional lung tissue with a diameter less than 3cm and without associated pneumonia, atelectasis (lung collapse) or lymphadenopathies (swollen lymph nodes).[13][10]
CT scan
For incidentally detected nodules on CT scan, Fleischner Society guidelines are given in table below. For multiple nodes, management is based on the most suspicious node.[8] These guidelines do not apply in lung cancer screening, in patients with immunosuppression, or in patients with known primary cancer.[8]
CT after 6–12 months to check if persistent, then after 2 years and then another 2 years
Part solid
No routine follow-up
CT after 6–12 months:
If unchanged and solid component remains <6mm: Annual CT for 5 years.
Solid component ≥6mm: highly suspicious
Multiple nodules
CT after 3–6 months. If stable, consider CT after 2 and then another 2 years.
CT after 3–6 months, then after 18–24 months
More frequent CT scans than what is recommended has not been shown to improve outcomes but will increase radiation exposure and the unnecessary health care can be expected to make the patient anxious and uncertain.[14]
PET scan
FDG-PET study of a 71-year-old woman with a solitary pulmonary nodule (thin arrow) in the left lower lobe near the heart. The scan also revealed abnormal increased activity at the gastro-esophageal junction (thick arrow). The final diagnosis was non-Hodgkin lymphoma at both sites.
If there is an intermediate risk of malignancy, further imaging with positron emission tomography (PET scan) is appropriate (if available). It can be done simultaneously as a CT scan in the form of PET-CT. Around 95% of patients with a malignant nodule will have an abnormal PET scan, while around 78% of patients with a benign nodule will look normal on PET (this is the test sensitivity and specificity).[15] Thus, an abnormal PET scan will reliably pick up cancer, but several other types of nodules (inflammatory or infectious, for example) will also show up on a PET scan. If the nodule has a diameter of less than one centimeter, PET scans are often avoided because of an increased risk of falsely normal results.[15][16][17] Cancerous lesions usually have a high metabolism on PET, as demonstrated by their high uptake of FDG (a radioactive sugar).
In selected cases, nodules can also be sampled through the airways using bronchoscopy or through the chest wall using fine-needle aspiration (which can be done under CT guidance). Needle aspiration can only retrieve groups of cells for cytology and not a tissue cylinder or biopsy, precluding evaluation of the tissue architecture. Theoretically, this makes the diagnosis of benign conditions more difficult, although rates higher than 90% have been reported.[20] Complications of the latter technique include hemorrhage into the lung and air leak in the pleural space between the lung and the chest wall (pneumothorax). However, not all these cases of pneumothorax need treatment with a chest tube.[21]
1 2 Ost D, Fein AM, Feinsilver SH (June 2003). "Clinical practice. The solitary pulmonary nodule". The New England Journal of Medicine. 348 (25): 2535–2542. doi:10.1056/NEJMcp012290. PMID12815140.
↑ Thiessen NR, Bremner R (October 2010). "The solitary pulmonary nodule: approach for a general surgeon". The Surgical Clinics of North America. 90 (5): 1003–1018. doi:10.1016/j.suc.2010.07.002. PMID20955880.
1 2 Jude CM, Nayak NB, Patel MK, Deshmukh M, Batra P (2014). "Pulmonary coccidioidomycosis: pictorial review of chest radiographic and CT findings". Radiographics. 34 (4): 912–925. doi:10.1148/rg.344130134. PMID25019431.
↑ Truong MT, Ko JP, Rossi SE, Rossi I, Viswanathan C, Bruzzi JF, etal. (October 2014). "Update in the evaluation of the solitary pulmonary nodule". Radiographics. 34 (6): 1658–1679. doi:10.1148/rg.346130092. PMID25310422.
1 2 Gould MK, Maclean CC, Kuschner WG, Rydzak CE, Owens DK (February 2001). "Accuracy of positron emission tomography for diagnosis of pulmonary nodules and mass lesions: a meta-analysis". JAMA. 285 (7): 914–924. doi:10.1001/jama.285.7.914. PMID11180735.
↑ Khan A (March 2007). "ACR Appropriateness Criteria on solitary pulmonary nodule". Journal of the American College of Radiology. 4 (3): 152–155. doi:10.1016/j.jacr.2006.12.003. PMID17412254.
↑ Vansteenkiste JF, Stroobants SS (January 2006). "PET scan in lung cancer: current recommendations and innovation". Journal of Thoracic Oncology. 1 (1): 71–73. doi:10.1097/01243894-200601000-00014. PMID17409830.
↑ Cronin P, Dwamena BA, Kelly AM, Carlos RC (March 2008). "Solitary pulmonary nodules: meta-analytic comparison of cross-sectional imaging modalities for diagnosis of malignancy". Radiology. 246 (3): 772–782. doi:10.1148/radiol.2463062148. PMID18235105.
↑ Klein JS, Salomon G, Stewart EA (March 1996). "Transthoracic needle biopsy with a coaxially placed 20-gauge automated cutting needle: results in 122 patients". Radiology. 198 (3): 715–720. doi:10.1148/radiology.198.3.8628859. PMID8628859.
A bone tumor is an abnormal growth of tissue in bone, traditionally classified as noncancerous (benign) or cancerous (malignant). Cancerous bone tumors usually originate from a cancer in another part of the body such as from lung, breast, thyroid, kidney and prostate. There may be a lump, pain, or neurological signs from pressure. A bone tumor might present with a pathologic fracture. Other symptoms may include fatigue, fever, weight loss, anemia and nausea. Sometimes there are no symptoms and the tumour is found when investigating another problem.
In medical or research imaging, an incidental imaging finding is an unanticipated finding which is not related to the original diagnostic inquiry. As with other types of incidental medical findings, they may represent a diagnostic, ethical, and philosophical dilemma because their significance is unclear. While some coincidental findings may lead to beneficial diagnoses, others may lead to overdiagnosis that results in unnecessary testing and treatment, sometimes called the "cascade effect".
A Pancoast tumor is a tumor of the apex of the lung. It is a type of lung cancer defined primarily by its location situated at the top end of either the right or left lung. It typically spreads to nearby tissues such as the ribs and vertebrae. Most Pancoast tumors are non-small-cell lung cancers.
Radiology (X-rays) is used in the diagnosis of tuberculosis. Abnormalities on chest radiographs may be suggestive of, but are never diagnostic of TB, but can be used to rule out pulmonary TB.
A benign tumor is a mass of cells (tumor) that does not invade neighboring tissue or metastasize. Compared to malignant (cancerous) tumors, benign tumors generally have a slower growth rate. Benign tumors have relatively well differentiated cells. They are often surrounded by an outer surface or stay contained within the epithelium. Common examples of benign tumors include moles and uterine fibroids.
A chest radiograph, called a chest X-ray (CXR), or chest film, is a projection radiograph of the chest used to diagnose conditions affecting the chest, its contents, and nearby structures. Chest radiographs are the most common film taken in medicine.
A hamartoma is a mostly benign, local malformation of cells that resembles a neoplasm of local tissue but is usually due to an overgrowth of multiple aberrant cells, with a basis in a systemic genetic condition, rather than a growth descended from a single mutated cell (monoclonality), as would typically define a benign neoplasm/tumor. Despite this, many hamartomas are found to have clonal chromosomal aberrations that are acquired through somatic mutations, and on this basis the term hamartoma is sometimes considered synonymous with neoplasm. Hamartomas are by definition benign, slow-growing or self-limiting, though the underlying condition may still predispose the individual towards malignancies.
Pleuropulmonary blastoma (PPB) is a rare cancer originating in the lung or pleural cavity. It occurs most often in infants and young children but also has been reported in adults. In a retrospective review of 204 children with lung tumors, pleuropulmonary blastoma and carcinoid tumor were the most common primary tumors. Pleuropulmonary blastoma is regarded as malignant. The male:female ratio is approximately one.
High-resolution computed tomography (HRCT) is a type of computed tomography (CT) with specific techniques to enhance image resolution. It is used in the diagnosis of various health problems, though most commonly for lung disease, by assessing the lung parenchyma. On the other hand, HRCT of the temporal bone is used to diagnose various middle ear diseases such as otitis media, cholesteatoma, and evaluations after ear operations.
Thyroid nodules are nodules which commonly arise within an otherwise normal thyroid gland. They may be hyperplastic or tumorous, but only a small percentage of thyroid tumors are malignant. Small, asymptomatic nodules are common, and often go unnoticed. Nodules that grow larger or produce symptoms may eventually need medical care. A goitre may have one nodule – uninodular, multiple nodules – multinodular, or be diffuse.
Lung cancer staging is the assessment of the extent to which a lung cancer has spread from its original source. As with most cancers, staging is an important determinant of treatment and prognosis. In general, more advanced stages of cancer are less amenable to treatment and have a worse prognosis.
Adenocarcinoma of the lung is the most common type of lung cancer, and like other forms of lung cancer, it is characterized by distinct cellular and molecular features. It is classified as one of several non-small cell lung cancers (NSCLC), to distinguish it from small cell lung cancer which has a different behavior and prognosis. Lung adenocarcinoma is further classified into several subtypes and variants. The signs and symptoms of this specific type of lung cancer are similar to other forms of lung cancer, and patients most commonly complain of persistent cough and shortness of breath.
Rheumatoid lung disease is a disease of the lung associated with RA, rheumatoid arthritis. Rheumatoid lung disease is characterized by pleural effusion, pulmonary fibrosis, lung nodules and pulmonary hypertension. Common symptoms associated with the disease include shortness of breath, cough, chest pain and fever. It is estimated that about one quarter of people with rheumatoid arthritis develop this disease, which are more likely to develop among elderly men with a history of smoking.
Tumor-like disorders of the lung pleura are a group of conditions that on initial radiological studies might be confused with malignant lesions. Radiologists must be aware of these conditions in order to avoid misdiagnosing patients. Examples of such lesions are: pleural plaques, thoracic splenosis, catamenial pneumothorax, pleural pseudotumor, diffuse pleural thickening, diffuse pulmonary lymphangiomatosis and Erdheim–Chester disease.
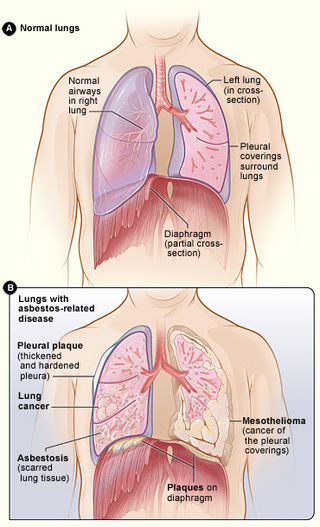
Asbestos-related diseases are disorders of the lung and pleura caused by the inhalation of asbestos fibres. Asbestos-related diseases include non-malignant disorders such as asbestosis, diffuse pleural thickening, pleural plaques, pleural effusion, rounded atelectasis and malignancies such as lung cancer and malignant mesothelioma.
Lung tumors are neoplastic lung nodules. These include:
Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH) is a diffuse parenchymal lung disease which often presents with symptoms of cough and shortness of breath. The pathological definition published by the World Health Organization is “a generalized proliferation of scattered single cells, small nodules, or linear proliferations of pulmonary neuroendocrine (PNE) cells that may be confined to the bronchial and bronchiolar epithelium.” The true prevalence of this disease is not known. To date, just under 200 cases have been reported in the literature. However, with an increase in recognition of this disease by radiologists and pulmonologists, the number of cases has been increasing. DIPNECH predominantly affects middle-aged women with slowly progressive lung obstruction. DIPNECH is usually discovered in one of two ways: 1) as an unexpected finding following a lung surgery; or 2) by evaluation of a patient in a pulmonary clinic with longstanding, unexplained symptoms.
Thoracic endometriosis is a rare form of endometriosis where endometrial-like tissue is found in the lung parenchyma and/or the pleura. It can be classified as either pulmonary, or pleural, respectively. Endometriosis is characterized by the presence of tissue similar to the lining of the uterus forming abnormal growths elsewhere in the body. Usually these growths are found in the pelvis, between the rectum and the uterus, the ligaments of the pelvis, the bladder, the ovaries, and the sigmoid colon. The cause is not known. The most common symptom of thoracic endometriosis is chest pain occurring right before or during menstruation. Diagnosis is based on clinical history and examination, augmented with X-ray, CT scan, and magnetic resonance imaging of the chest. Treatment options include surgery and hormones.
Pulmonary sclerosing pneumocytoma is a rare benign tumour of the lung.
A lung cavity or pulmonary cavity is an abnormal, thick-walled, air-filled space within the lung. Cavities in the lung can be caused by infections, cancer, autoimmune conditions, trauma, congenital defects, or pulmonary embolism. The most common cause of a single lung cavity is lung cancer. Bacterial, mycobacterial, and fungal infections are common causes of lung cavities. Globally, tuberculosis is likely the most common infectious cause of lung cavities. Less commonly, parasitic infections can cause cavities. Viral infections almost never cause cavities. The terms cavity and cyst are frequently used interchangeably; however, a cavity is thick walled, while a cyst is thin walled. The distinction is important because cystic lesions are unlikely to be cancer, while cavitary lesions are often caused by cancer.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.