
A pandemic is an epidemic of an infectious disease that has spread across a large region, for instance multiple continents or worldwide, affecting a substantial number of individuals. Widespread endemic diseases with a stable number of infected individuals such as recurrences of seasonal influenza are generally excluded as they occur simultaneously in large regions of the globe rather than being spread worldwide.
The UK statutory notification system for infectious diseases is a system whereby doctors are required to notify a "proper officer" of the local authority if they are presented with a case of a serious infectious disease such as diphtheria or measles. The proper officer then sends a report to the Centre for Infections of the Health Protection Agency (HPA) in Colindale, north London.
The Public Health Agency of Canada is an agency of the Government of Canada that is responsible for public health, emergency preparedness and response, and infectious and chronic disease control and prevention.
The Hong Kong flu, also known as the 1968 flu pandemic, was a flu pandemic that occurred in 1968 and 1969 and which killed between one and four million people globally. It is among the deadliest pandemics in history, and was caused by an H3N2 strain of the influenza A virus. The virus was descended from H2N2 through antigenic shift, a genetic process in which genes from multiple subtypes are reassorted to form a new virus.

Waterborne diseases are conditions caused by pathogenic micro-organisms that are transmitted by water. These diseases can be spread while bathing, washing, drinking water, or by eating food exposed to contaminated water. They are a pressing issue in rural areas amongst developing countries all over the world. While diarrhea and vomiting are the most commonly reported symptoms of waterborne illness, other symptoms can include skin, ear, respiratory, or eye problems. Lack of clean water supply, sanitation and hygiene (WASH) are major causes for the spread of waterborne diseases in a community. Therefore, reliable access to clean drinking water and sanitation is the main method to prevent waterborne diseases.
Public health informatics has been defined as the systematic application of information and computer science and technology to public health practice, research, and learning. It is one of the subdomains of health informatics.
Disease surveillance is an epidemiological practice by which the spread of disease is monitored in order to establish patterns of progression. The main role of disease surveillance is to predict, observe, and minimize the harm caused by outbreak, epidemic, and pandemic situations, as well as increase knowledge about which factors contribute to such circumstances. A key part of modern disease surveillance is the practice of disease case reporting.
HIV/AIDS in China can be traced to an initial outbreak of the human immunodeficiency virus (HIV) first recognized in 1989 among injecting drug users along China's southern border. Figures from the Chinese Center for Disease Control and Prevention, World Health Organization, and UNAIDS estimate that there were 1.25 million people living with HIV/AIDS in China at the end of 2018, with 135,000 new infections from 2017. The reported incidence of HIV/AIDS in China is relatively low, but the Chinese government anticipates that the number of individuals infected annually will continue to increase.
A notifiable disease is any disease that is required by law to be reported to government authorities. The collation of information allows the authorities to monitor the disease, and provides early warning of possible outbreaks. In the case of livestock diseases, there may also be the legal requirement to kill the infected livestock upon notification. Many governments have enacted regulations for reporting of both human and animal diseases.
The Centers for Disease Control and Prevention, formed in 1946, is the leading national public health institute of the United States. It is a United States federal agency, under the United States Department of Health and Human Services. Its main goal is to protect public health and safety through the control and prevention of disease, injury, and disability in the US and internationally.

Polio eradication, the permanent global cessation of circulation of the poliovirus and hence elimination of the poliomyelitis (polio) it causes, is the aim of a multinational public health effort begun in 1988, led by the World Health Organization (WHO), the United Nations Children's Fund (UNICEF) and the Rotary Foundation. These organizations, along with the U.S. Centers for Disease Control and Prevention (CDC) and The Gates Foundation, have spearheaded the campaign through the Global Polio Eradication Initiative (GPEI). Successful eradication of infectious diseases has been achieved twice before, with smallpox in humans and rinderpest in ruminants.

Program for Monitoring Emerging Diseases is among the largest publicly available emerging diseases and outbreak reporting systems in the world. The purpose of ProMED is to promote communication amongst the international infectious disease community, including scientists, physicians, veterinarians, epidemiologists, public health professionals, and others interested in infectious diseases on a global scale. Founded in 1994, ProMED has pioneered the concept of electronic, Internet-based emerging disease and outbreak detection reporting. In 1999, ProMED became a program of the International Society for Infectious Diseases. As of 2016, ProMED has more than 75,000 subscribers in over 185 countries. With an average of 13 posts per day, ProMED provides users with up-to-date information concerning infectious disease outbreaks on a global scale.
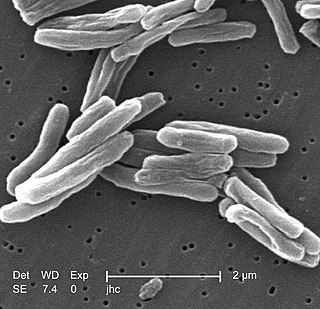
Tuberculosis is a serious public health problem in China. China has the world's third largest cases of tuberculosis, but progress in tuberculosis control was slow during the 1990s. Detection of tuberculosis had stagnated at around 30% of the estimated total of new cases, and multidrug-resistant tuberculosis was a major problem. These signs of inadequate tuberculosis control can be linked to a malfunctioning health system. The spread of severe acute respiratory syndrome (SARS) in 2003, brought to light substantial weaknesses in the country's public health system. After the government realized the impact that the SARS outbreak had on the country, they increased leadership in their health department. After the SARS epidemic was brought under control, the government increased its commitment and leadership to tackle public health problems and, among other efforts, increased public health funding, revised laws that concerned the control of infectious diseases, implemented the world's largest internet-based disease reporting system to improve transparency, reach and speed, and started a program to rebuild local public health facilities and national infrastructure.
Chronic, non-communicable diseases account for an estimated 80% of total deaths and 70% of disability-adjusted life years (DALYs) lost in China. Cardiovascular diseases, chronic respiratory disease, and cancer are the leading causes of both death and of the burden of disease, and exposure to risk factors is high: more than 300 million men smoke cigarettes and 160 million adults are hypertensive, most of whom are not being treated. An obesity epidemic is imminent, with more than 20% of children aged 7–17 years in big cities now overweight or obese. Rates of death from chronic disease in middle-aged people are higher in China than in some high-income countries.

Measles vaccine protects against becoming infected with measles. Nearly all of those who do not develop immunity after a single dose develop it after a second dose. When the rate of vaccination within a population is greater than 92%, outbreaks of measles typically no longer occur; however, they may occur again if the rate of vaccination decreases. The vaccine's effectiveness lasts many years. It is unclear if it becomes less effective over time. The vaccine may also protect against measles if given within a couple of days after exposure to measles.
The Australian Measles Control Campaign was initiated in August 1998 as part of the World Health Organization's global measles eradication program, and in response to major epidemics in Australia throughout 1994/95, together with a report predicting another impending measles epidemic in Australia. The campaign vaccinated 1.78 million children, making it the largest national vaccination campaign conducted in Australia since the introduction of poliomyelitis vaccination in 1956.

On 20 January 2016, the health minister of Angola reported 23 cases of yellow fever with 7 deaths among Eritrean and Congolese citizens living in Angola in Viana municipality, a suburb of the capital of Luanda. The first cases were reported in Eritrean visitors beginning on 5 December 2015 and confirmed by the Pasteur WHO reference laboratory in Dakar, Senegal in January. The outbreak was classified as an urban cycle of yellow fever transmission, which can spread rapidly. A preliminary finding that the strain of the yellow fever virus was closely related to a strain identified in a 1971 outbreak in Angola was confirmed in August 2016. Moderators from ProMED-mail stressed the importance of initiating a vaccination campaign immediately to prevent further spread. The CDC classified the outbreak as Watch Level 2 on 7 April 2016. The WHO declared it a grade 2 event on its emergency response framework having moderate public health consequences.
The Health Protection Surveillance Centre (HPSC) is part of Ireland's Health Service Executive.

Outbreak response or outbreak control measures are acts which attempt to minimize the spread of or effects of a disease outbreak. Outbreak response includes aspects of general disease control such as maintaining adequate hygiene, but may also include responses that extend beyond traditional healthcare settings and are unique to an outbreak, such as physical distancing, contact tracing, mapping of disease clusters, or quarantine. Some measures such as isolation are also useful in preventing an outbreak from occurring in the first place.

The 1957–1958 Asian flu pandemic was a global pandemic of influenza A virus subtype H2N2 that originated in Guizhou in Southern China. The number of excess deaths caused by the pandemic is estimated to be 1–4 million around the world, making it one of the deadliest pandemics in history. A decade later, a reassorted viral strain H3N2 further caused the Hong Kong flu pandemic (1968–1969).