
Bornholm disease, also known as epidemic pleurodynia, is a condition characterized by myositis of the abdomen or chest caused by the Coxsackie B virus or other viruses. The myositis manifests as an intermittent stabbing pain in the musculature that is seen primarily in children and young adults.

Hand, foot, and mouth disease (HFMD) is a common infection caused by a group of enteroviruses. It typically begins with a fever and feeling generally unwell. This is followed a day or two later by flat discolored spots or bumps that may blister, on the hands, feet and mouth and occasionally buttocks and groin. Signs and symptoms normally appear 3–6 days after exposure to the virus. The rash generally resolves on its own in about a week. Fingernail and toenail loss may occur a few weeks later, but they will regrow with time.
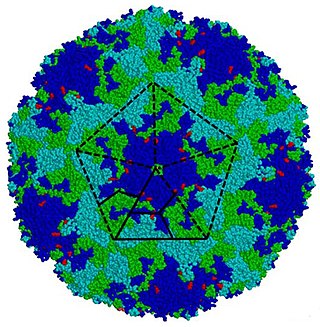
Coxsackie B4 virus are enteroviruses that belong to the Picornaviridae family. These viruses can be found worldwide. They are positive-sense, single-stranded, non-enveloped RNA viruses with icosahedral geometry. Coxsackieviruses have two groups, A and B, each associated with different diseases. Coxsackievirus group A is known for causing hand-foot-and-mouth diseases while Group B, which contains six serotypes, can cause a varying range of symptoms like gastrointestinal distress myocarditis. Coxsackievirus B4 has a cell tropism for natural killer cells and pancreatic islet cells. Infection can lead to beta cell apoptosis which increases the risk of insulitis.

Fifth disease, also known as erythema infectiosum and slapped cheek syndrome, is a common and contagious disease caused by infection from parvovirus B19. This virus was discovered in 1975 and can cause other diseases besides fifth disease. Fifth disease typically presents as a rash and is most common in children. While parvovirus B19 can affect people of all ages, only two out of ten individuals will present with symptoms.
Coxsackieviruses are a few related enteroviruses that belong to the Picornaviridae family of nonenveloped, linear, positive-sense single-stranded RNA viruses, as well as its genus Enterovirus, which also includes poliovirus and echovirus. Enteroviruses are among the most common and important human pathogens, and ordinarily its members are transmitted by the fecal–oral route. Coxsackieviruses share many characteristics with poliovirus. With control of poliovirus infections in much of the world, more attention has been focused on understanding the nonpolio enteroviruses such as coxsackievirus.
Coxsackie B is a group of six serotypes of coxsackievirus (CVB1-CVB6), a pathogenic enterovirus, that trigger illness ranging from gastrointestinal distress to full-fledged pericarditis and myocarditis.
Enterovirus is a genus of positive-sense single-stranded RNA viruses associated with several human and mammalian diseases. Enteroviruses are named by their transmission-route through the intestine.

Gingivostomatitis is a combination of gingivitis and stomatitis, or an inflammation of the oral mucosa and gingiva. Herpetic gingivostomatitis is often the initial presentation during the first ("primary") herpes simplex infection. It is of greater severity than herpes labialis which is often the subsequent presentations. Primary herpetic gingivostomatitis is the most common viral infection of the mouth.

Adenovirus infection is a contagious viral disease, caused by adenoviruses, commonly resulting in a respiratory tract infection. Typical symptoms range from those of a common cold, such as nasal congestion, coryza and cough, to difficulty breathing as in pneumonia. Other general symptoms include fever, fatigue, muscle aches, headache, abdominal pain and swollen neck glands. Onset is usually two to fourteen days after exposure to the virus. A mild eye infection may occur on its own, combined with a sore throat and fever, or as a more severe adenoviral keratoconjunctivitis with a painful red eye, intolerance to light and discharge. Very young children may just have an earache. Adenovirus infection can present as a gastroenteritis with vomiting, diarrhoea and abdominal pain, with or without respiratory symptoms. However, some people have no symptoms.

The schedule for childhood immunizations in the United States is published by the Centers for Disease Control and Prevention (CDC). The vaccination schedule is broken down by age: birth to six years of age, seven to eighteen, and adults nineteen and older. Childhood immunizations are key in preventing diseases with epidemic potential.
Herpes gladiatorum is one of the most infectious of herpes-caused diseases, and is transmissible by skin-to-skin contact. The disease was first described in the 1960s in the New England Journal of Medicine. It is caused by contagious infection with human herpes simplex virus type 1 (HSV-1), which more commonly causes oral herpes. Another strain, HSV-2 usually causes genital herpes, although the strains are very similar and either can cause herpes in any location.
Enterovirus 71 (EV71), also known as Enterovirus A71 (EV-A71), is a virus of the genus Enterovirus in the Picornaviridae family, notable for its role in causing epidemics of severe neurological disease and hand, foot, and mouth disease in children. It was first isolated and characterized from cases of neurological disease in California in 1969. Enterovirus 71 infrequently causes polio-like syndrome permanent paralysis.

Chickenpox, also known as varicella, is a highly contagious, vaccine-preventable disease caused by the initial infection with varicella zoster virus (VZV), a member of the herpesvirus family. The disease results in a characteristic skin rash that forms small, itchy blisters, which eventually scab over. It usually starts on the chest, back, and face. It then spreads to the rest of the body. The rash and other symptoms, such as fever, tiredness, and headaches, usually last five to seven days. Complications may occasionally include pneumonia, inflammation of the brain, and bacterial skin infections. The disease is usually more severe in adults than in children.

A cold sore is a type of herpes infection caused by the herpes simplex virus that affects primarily the lip. Symptoms typically include a burning pain followed by small blisters or sores. The first attack may also be accompanied by fever, sore throat, and enlarged lymph nodes. The rash usually heals within ten days, but the virus remains dormant in the trigeminal ganglion. The virus may periodically reactivate to create another outbreak of sores in the mouth or lip.
sCAR-Fc is an experimental prophylactic treatment against coxsackievirus B3 (CVB) infections. Coxsackievirus B3 can cause cardiac damage, eventually resulting in a weakened and enlarged heart that is termed dilated cardiomyopathy. While many other treatments inhibit viral proliferation in myocytes, sCAR-Fc prevents the virus entering the cell by competitively binding to coxsackie virus and adenovirus receptors (CAR) on the membrane of myocytes.
Coxsackieviruses-induced cardiomyopathy are positive-stranded RNA viruses in picornavirus family and the genus enterovirus, acute enterovirus infections such as Coxsackievirus B3 have been identified as the cause of virally induced acute myocarditis, resulting in dilated cardiomyopathy. Dilated cardiomyopathy in humans can be caused by multiple factors including hereditary defects in the cytoskeletal protein dystrophin in Duchenne muscular dystrophy (DMD) patients). A heart that undergoes dilated cardiomyopathy shows unique enlargement of ventricles, and thinning of the ventricular wall that may lead to heart failure. In addition to the genetic defects in dystrophin or other cytoskeletal proteins, a subset of dilated cardiomyopathy is linked to enteroviral infection in the heart, especially coxsackievirus B. Enterovirus infections are responsible for about 30% of the cases of acquired dilated cardiomyopathy in humans.
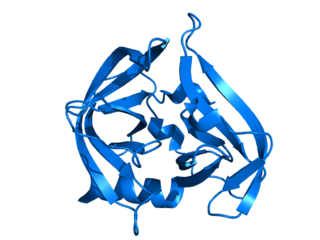
Picornain 3C is a protease found in picornaviruses, which cleaves peptide bonds of non-terminal sequences. Picornain 3C’s endopeptidase activity is primarily responsible for the catalytic process of selectively cleaving Gln-Gly bonds in the polyprotein of poliovirus and with substitution of Glu for Gln, and Ser or Thr for Gly in other picornaviruses. Picornain 3C are cysteine proteases related by amino acid sequence to trypsin-like serine proteases. Picornain 3C is encoded by enteroviruses, rhinoviruses, aphtoviruses and cardioviruses. These genera of picoviruses cause a wide range of infections in humans and mammals.

Acute flaccid myelitis (AFM) is a serious condition of the spinal cord. Symptoms include rapid onset of arm or leg weakness and decreased reflexes. Difficulty moving the eyes, speaking, or swallowing may also occur. Occasionally, numbness or pain may be present. Complications can include trouble breathing.
Beginning in January 2018, an outbreak of hand, foot, and mouth disease (HFMD) occurred among children nationwide across Malaysia. Nearly 38,000 cases were recorded between January 1 and July 26, and by August 14 the total number of cases had risen to 51,000. Among the states and federal territories affected by the outbreak, Selangor recorded the highest cases with 11,349, Kuala Lumpur with 4,428 and Sarawak with 4,412 cases as reported in July 2018. At least two children in Sarawak and Penang died from complications caused by the virus.
The 1997 Sarawak HFMD outbreak is a hand, foot, and mouth disease (HFMD) outbreak from April until June caused by the Enterovirus 71 (EV-71) affecting 600 children in the state of Sarawak in Malaysia. Sarawak is the first state in Malaysia that reported HFMD outbreak. An estimated 28 to 31 of the infected children died as a result. The affected children are aged between five months to six years.

