
Amniocentesis is a medical procedure used primarily in the prenatal diagnosis of genetic conditions. It has other uses such as in the assessment of infection and fetal lung maturity. Prenatal diagnostic testing, which includes amniocentesis, is necessary to conclusively diagnose the majority of genetic disorders, with amniocentesis being the gold-standard procedure after 15 weeks' gestation.

The ankle, the talocrural region or the jumping bone (informal) is the area where the foot and the leg meet. The ankle includes three joints: the ankle joint proper or talocrural joint, the subtalar joint, and the inferior tibiofibular joint. The movements produced at this joint are dorsiflexion and plantarflexion of the foot. In common usage, the term ankle refers exclusively to the ankle region. In medical terminology, "ankle" can refer broadly to the region or specifically to the talocrural joint.

The Achilles tendon or heel cord, also known as the calcaneal tendon, is a tendon at the back of the lower leg, and is the thickest in the human body. It serves to attach the plantaris, gastrocnemius (calf) and soleus muscles to the calcaneus (heel) bone. These muscles, acting via the tendon, cause plantar flexion of the foot at the ankle joint, and flexion at the knee.

Kyphosis is an abnormally excessive convex curvature of the spine as it occurs in the thoracic and sacral regions. Abnormal inward concave lordotic curving of the cervical and lumbar regions of the spine is called lordosis.
Pes cavus, also known as high arch, is an orthopedic condition that presents as a hollow arch underneath the foot with a pronounced high ridge at the top when weight bearing.

An omphalocele or omphalocoele, also known as an exomphalos, is a rare abdominal wall defect. Beginning at the 6th week of development, rapid elongation of the gut and increased liver size reduces intra abdominal space, which pushes intestinal loops out of the abdominal cavity. Around 10th week, the intestine returns to the abdominal cavity and the process is completed by the 12th week. Persistence of intestine or the presence of other abdominal viscera in the umbilical cord results in an omphalocele.

Arthrogryposis (AMC) describes congenital joint contracture in two or more areas of the body. It derives its name from Greek, literally meaning 'curving of joints'.

Flat feet, also called pes planus or fallen arches, is a postural deformity in which the arches of the foot collapse, with the entire sole of the foot coming into complete or near-complete contact with the ground. Sometimes children are born with flat feet (congenital). There is a functional relationship between the structure of the arch of the foot and the biomechanics of the lower leg. The arch provides an elastic, springy connection between the forefoot and the hind foot so that a majority of the forces incurred during weight bearing on the foot can be dissipated before the force reaches the long bones of the leg and thigh.
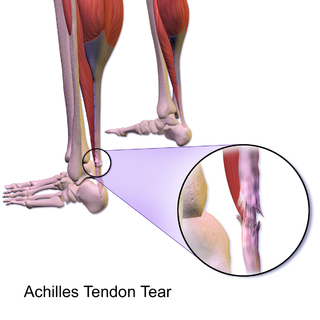
Achilles tendon rupture is when the Achilles tendon, at the back of the ankle, breaks. Symptoms include the sudden onset of sharp pain in the heel. A snapping sound may be heard as the tendon breaks and walking becomes difficult.

In pathology, a contracture is a shortening of muscles, tendons, skin, and nearby soft tissues that causes the joints to shorten and become very stiff, preventing normal movement. A contracture is usually permanent, but less commonly can be temporary, or resolve over time but reoccur later in life.
Foot and ankle surgery is a sub-specialty of orthopedics and podiatry that deals with the treatment, diagnosis and prevention of disorders of the foot and ankle. Orthopaedic surgeons are medically qualified, having been through four years of college, followed by 4 years of medical school or osteopathic medical school to obtain an M.D. or D.O. followed by specialist training as a resident in orthopaedics, and only then do they sub-specialise in foot and ankle surgery. Training for a podiatric foot and ankle surgeon consists of four years of college, four years of podiatric medical school (D.P.M.), 3–4 years of a surgical residency and an optional 1 year fellowship.

Toe walking is a term describing a type of walking style. Toe walking is when a person walks on their toes or the ball of their foot, without putting much or any weight on the heel or any other part of the foot. Toe walking in toddlers is common. Children who toe walk as toddlers commonly adopt a heel-toe walking pattern as they grow older. If a child continues to walk on their toes past the age of three, or cannot get their heels to the ground at all, they should be examined by a health professional who is experienced in assessing children's walking.

Ignacio Ponseti, also known as Ignasi Ponsetí i Vives, was a Spanish-American physician, specializing in orthopedics. He was born on 3 June 1914 in Menorca, part of the Balearic Islands, Spain, Ponseti was the son of a watchmaker and spent his childhood helping repair watches. This skill was said to eventually contribute to his abilities as an orthopedist. He served three years as a medic during the Spanish Civil War treating orthopedic injuries of wounded soldiers. He left Spain shortly after the end of the war and became a faculty member and practicing physician at the University of Iowa, where he developed his ground-breaking, non-surgical treatment for the clubfoot defect - the Ponseti Method.
The Ponseti method is a manipulative technique that corrects congenital clubfoot without invasive surgery. It was developed by Ignacio V. Ponseti of the University of Iowa Hospitals and Clinics, US, in the 1950s, and was repopularized in 2000 by John Herzenberg in the US and Europe and in Africa by NHS surgeon Steve Mannion. It is a standard treatment for clubfoot.
A tenotomy is a surgical act which involves the division of a tendon. It and related procedures are also referred to as tendon release, tendon lengthening, and heel-cord release.
Unlike the flexible flat foot that is commonly encountered in young children, congenital vertical talus is characterized by presence of a very rigid foot deformity. The foot deformity in congenital vertical talus consists of various components, namely a prominent calcaneus caused by the ankle equines or plantar flexion, a convex and rounded sole of the foot caused by prominence of the head of the talus, and a dorsiflexion and abduction of the forefoot and midfoot on the hindfoot. It gets its name from the foot's resemblance to the bottom of a rocking chair. There are two subcategories of congenital vertical talus; namely idiopathic or isolated type, and non-idiopathic type, which may be seen in association with arthrogryposis multiplex congenital, genetic syndromes and other neuromuscular disorders.

Comparative foot morphology involves comparing the form of distal limb structures of a variety of terrestrial vertebrates. Understanding the role that the foot plays for each type of organism must take account of the differences in body type, foot shape, arrangement of structures, loading conditions and other variables. However, similarities also exist among the feet of many different terrestrial vertebrates. The paw of the dog, the hoof of the horse, the manus (forefoot) and pes (hindfoot) of the elephant, and the foot of the human all share some common features of structure, organization and function. Their foot structures function as the load-transmission platform which is essential to balance, standing and types of locomotion.
Children's feet are smaller than those of adults, not reaching full size until the ages of 13 in girls and 15 in boys. There are correspondingly small sizes of shoes for them. In poor populations and tropical countries, children commonly go barefoot.

Congenital clasped thumb describes an anomaly which is characterized by a fixed thumb into the palm at the metacarpophalangeal joint in one or both hands. The incidence and genetic background are unknown. A study of Weckesser et al. showed that boys are twice as often affected with congenital clasped thumb compared to girls. The anomaly is in most cases bilateral . A congenital clasped thumb can be an isolated anomaly, but can also be attributed to several syndromes.
The management of scoliosis is complex and is determined primarily by the type of scoliosis encountered: syndromic, congenital, neuromuscular, or idiopathic. Treatment options for idiopathic scoliosis are determined in part by the severity of the curvature and skeletal maturity, which together help predict the likelihood of progression. Non-surgical treatment should be pro-active with intervention performed early as "Best results were obtained in 10-25 degrees scoliosis which is a good indication to start therapy before more structural changes within the spine establish." Treatment options have historically been categorized under the following types:
- Observation
- Bracing
- Specialized physical therapy
- Surgery







