
Infant formula, also called baby formula, simply formula, baby milk or infant milk, is designed and marketed for feeding to babies and infants under 12 months of age, usually prepared for bottle-feeding or cup-feeding from powder or liquid. The U.S. Federal Food, Drug, and Cosmetic Act (FFDCA) defines infant formula as "a food which purports to be or is represented for special dietary use solely as a food for infants by reason of its simulation of human milk or its suitability as a complete or partial substitute for human milk".
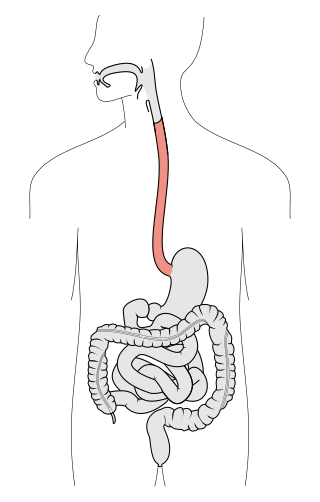
Swallowing, also called deglutition or inglutition in scientific contexts, is the process in the body of a human that allows for a substance to pass from the mouth, to the pharynx, and into the esophagus, while shutting the epiglottis. Swallowing is an important part of eating and drinking. If the process fails and the material goes through the trachea, then choking or pulmonary aspiration can occur. In the human body the automatic temporary closing of the epiglottis is controlled by the swallowing reflex.

A baby bottle, nursing bottle, or feeding bottle is a bottle with a teat attached to it, which creates the ability to drink via suckling. It is typically used by infants and young children, or if someone cannot drink from a cup, for feeding oneself or being fed. It can also be used to feed non-human mammals.

Weaning is the process of gradually introducing an infant human or other mammal to what will be its adult diet while withdrawing the supply of its mother's milk. In the UK, weaning primarily refers to the introduction of solid foods at 6 months; in the US, it primarily refers to stopping breastfeeding.
The pharyngeal reflex or gag reflex is a reflex muscular contraction of the back of the throat, evoked by touching the roof of the mouth, back of the tongue, area around the tonsils, uvula, and back of the throat. It, along with other aerodigestive reflexes such as reflexive pharyngeal swallowing, prevents objects in the oral cavity from entering the throat except as part of normal swallowing and helps prevent choking, and is a form of coughing. The pharyngeal reflex is different from the laryngeal spasm, which is a reflex muscular contraction of the vocal cords.

Chewing or mastication is the process by which food is crushed and ground by the teeth. It is the first step in the process of digestion, allowing a greater surface area for digestive enzymes to break down the foods.

Breast milk or mother's milk is milk produced by the mammary glands in the breast of human females. Breast milk is the primary source of nutrition for newborn infants, comprising fats, proteins, carbohydrates, and a varying composition of minerals and vitamins. Breast milk also contains substances that help protect an infant against infection and inflammation, such as symbiotic bacteria and other microorganisms and immunoglobulin A, whilst also contributing to the healthy development of the infant's immune system and gut microbiome.

Baby food is any soft, easily consumed food other than breastmilk or infant formula that is made specifically for human babies between six months and two years old. The food comes in many varieties and flavors that are purchased ready-made from producers, or it may be table food eaten by the family that has been mashed or otherwise broken down.
Oropharyngeal dysphagia is the inability to empty material from the oropharynx into the esophagus as a result of malfunction near the esophagus. Oropharyngeal dysphagia manifests differently depending on the underlying pathology and the nature of the symptoms. Patients with dysphagia can experience feelings of food sticking to their throats, coughing and choking, weight loss, recurring chest infections, or regurgitation. Depending on the underlying cause, age, and environment, dysphagia prevalence varies. In research including the general population, the estimated frequency of oropharyngeal dysphagia has ranged from 2 to 16 percent.
Erotic lactation is sexual arousal by sucking on a female or male breast. Depending on the context, the practice can also be referred to as adult suckling, adult nursing, and adult breastfeeding. Practitioners sometimes refer to themselves as being in an adult nursing relationship (ANR). Two persons in an exclusive relationship can be called a nursing couple
Overactive let-down (OALD) is the forceful ejection of milk from the breast during breastfeeding. In some women it occurs only with the first let-down in a feeding, occasionally women may have multiple strong letdowns during a feeding. OALD can make breastfeeding difficult and can be the source of some breastfeeding complications. It may also be known as hyper milk-ejection. A woman may have OALD in addition to an oversupply of breastmilk. The physical or medical cause of an overactive let-down is still unknown. Whether mothers with OALD have a higher overall milk volume – or a strong reaction to the hormone oxytocin also remains to be seen.

Breastfeeding difficulties refers to problems that arise from breastfeeding, the feeding of an infant or young child with milk from a woman's breasts. Although babies have a sucking reflex that enables them to suck and swallow milk, and human breast milk is usually the best source of nourishment for human infants, there are circumstances under which breastfeeding can be problematic, or even in rare instances, contraindicated.

Breastfeeding, also known as nursing, is the process where breast milk is fed to a child. Breast milk may be from the breast, or may be pumped and fed to the infant. The World Health Organization (WHO) recommend that breastfeeding begin within the first hour of a baby's birth and continue as the baby wants. Health organizations, including the WHO, recommend breastfeeding exclusively for six months. This means that no other foods or drinks, other than vitamin D, are typically given. The WHO recommends exclusive breastfeeding for the first 6 months of life, followed by continued breastfeeding with appropriate complementary foods for up to 2 years and beyond. Of the 135 million babies born every year, only 42% are breastfed within the first hour of life, only 38% of mothers practice exclusive breastfeeding during the first six months, and 58% of mothers continue breastfeeding up to the age of two years and beyond.
A feeding disorder, in infancy or early childhood, is a child's refusal to eat certain food groups, textures, solids or liquids for a period of at least one month, which causes the child to not gain enough weight, grow naturally or cause any developmental delays. Feeding disorders resemble failure to thrive, except that at times in feeding disorder there is no medical or physiological condition that can explain the very small amount of food the children consume or their lack of growth. Some of the times, a previous medical condition that has been resolved is causing the issue.
Premastication, pre-chewing, or kiss feeding is the act of chewing food for the purpose of physically breaking it down in order to feed another that is incapable of masticating the food by themselves. This is often done by the mother or relatives of a baby to produce baby food capable of being consumed by the child during the weaning process. The chewed food in the form of a bolus is transferred from the mouth of one individual to another, either directly mouth-to-mouth, via utensils, hands, or is further cooked or processed prior to feeding.
Infant feeding is the practice of feeding infants. Breast milk provides the best nutrition when compared to infant formula. Infants are usually introduced to solid foods at around four to six months of age.

Foodborne illness is any illness resulting from the food spoilage of contaminated food, pathogenic bacteria, viruses, or parasites that contaminate food. Infant food safety is the identification of risky food handling practices and the prevention of illness in infants. Foodborne illness is a serious health issue, especially for babies and children. Infants and young children are particularly vulnerable to foodborne illness because their immune systems are not developed enough to fight off foodborne bacterial infections. In fact, 800,000 illnesses affect children under the age of 10 in the U.S. each year. Therefore, extra care should be taken when handling and preparing their food.
Toddler nutrition is the description of the dietary needs of toddlers aged one to two years old. Food provides the energy and nutrients that toddlers need to be healthy. An adequate intake in nutrient rich food is good nutrition. A diet lacking essential calories, minerals, fluid and vitamins could be considered 'bad' nutrition. Nutrition needs are different for toddlers. For a baby, breast milk is "best" and it has all the necessary vitamins and minerals. Toddlers typically have been weaned from breast milk and infant formula. Though infants usually start eating solid foods between 4 and 6 months of age, more and more solid foods are consumed by a growing toddler. If a food introduced one at a time, a potential allergen can be identified. Food provides the energy and nutrients that young children need to be healthy. Toddlers are learning to feed themselves and to eat new foods. They should eat a variety of foods from all the food groups. Each day, toddlers need enough nutrients, including

Establishment of breastfeeding refers to the initiation of providing breast milk of mother to baby. According to the World Health Organization(WHO), breastfeeding is the best way to provide nourishment, including essential nutrients, energy and antibodies, to infants and toddlers. The start of breastfeeding is supported by the milk production which depends on the development of internal and external breast structure and hormonal control on milk secretion. Besides milk supply, adopting the correct approach of breastfeeding helps build up the maternal bond, which in turn promotes breastfeeding. Not only does nursing strengthen the mother-child relationship, but it also improves the intelligence and immunity of breastfed children and diminishes breastfeeding mothers' risks to have ovarian and breast cancer.
Anne-Louise M. Heath is a New Zealand academic, and is a full professor at the University of Otago, specialising in baby and infant nutrition, including baby-led weaning and iron deficiency.
Case-Smith, J & Humphry, R. (2005). Feeding Intervention. In J.Case-Smith (Ed.), Occupational therapy for children (pp. 481–520). St Louis, MO: Elsevier.
Morris, S.E, & Dunn-Klein, M.(2000).Pre-feeding skills: A comprehensive resource for mealtime development (2nd ed.). Austin, TX: PRO-ED, Inc.
Rapley, G. & Murkett, T. (2005). Baby Led Weaning: the essential guide to introducing solid foods and helping your baby to grow up a happy and confident eater. New York, NY: The experiment, LLC.