
The aorta is the main and largest artery in the human body, originating from the left ventricle of the heart, branching upwards immediately after, and extending down to the abdomen, where it splits at the aortic bifurcation into two smaller arteries. The aorta distributes oxygenated blood to all parts of the body through the systemic circulation.

The aortic valve is a valve in the heart of humans and most other animals, located between the left ventricle and the aorta. It is one of the four valves of the heart and one of the two semilunar valves, the other being the pulmonary valve. The aortic valve normally has three cusps or leaflets, although in 1–2% of the population it is found to congenitally have two leaflets. The aortic valve is the last structure in the heart the blood travels through before stopping the flow through the systemic circulation.
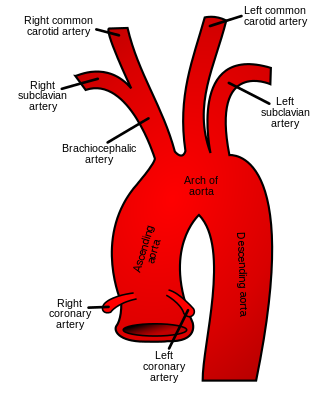
The brachiocephalic artery, brachiocephalic trunk, or innominate artery is an artery of the mediastinum that supplies blood to the right arm, head, and neck.

Aortic dissection (AD) occurs when an injury to the innermost layer of the aorta allows blood to flow between the layers of the aortic wall, forcing the layers apart. In most cases, this is associated with a sudden onset of agonizing chest or back pain, often described as "tearing" in character. Vomiting, sweating, and lightheadedness may also occur. Damage to other organs may result from the decreased blood supply, such as stroke, lower extremity ischemia, or mesenteric ischemia. Aortic dissection can quickly lead to death from insufficient blood flow to the heart or complete rupture of the aorta.
A pulmonary artery is an artery in the pulmonary circulation that carries deoxygenated blood from the right side of the heart to the lungs. The largest pulmonary artery is the main pulmonary artery or pulmonary trunk from the heart, and the smallest ones are the arterioles, which lead to the capillaries that surround the pulmonary alveoli.

Vascular surgery is a surgical subspecialty in which vascular diseases involving the arteries, veins, or lymphatic vessels, are managed by medical therapy, minimally-invasive catheter procedures and surgical reconstruction. The specialty evolved from general and cardiovascular surgery where it refined the management of just the vessels, no longer treating the heart or other organs. Modern vascular surgery includes open surgery techniques, endovascular techniques and medical management of vascular diseases - unlike the parent specialities. The vascular surgeon is trained in the diagnosis and management of diseases affecting all parts of the vascular system excluding the coronaries and intracranial vasculature. Vascular surgeons also are called to assist other physicians to carry out surgery near vessels, or to salvage vascular injuries that include hemorrhage control, dissection, occlusion or simply for safe exposure of vascular structures.

Bicuspid aortic valve (BAV) is a form of heart disease in which two of the leaflets of the aortic valve fuse during development in the womb resulting in a two-leaflet (bicuspid) valve instead of the normal three-leaflet (tricuspid) valve. BAV is the most common cause of heart disease present at birth and affects approximately 1.3% of adults. Normally, the mitral valve is the only bicuspid valve and this is situated between the heart's left atrium and left ventricle. Heart valves play a crucial role in ensuring the unidirectional flow of blood from the atria to the ventricles, or from the ventricle to the aorta or pulmonary trunk. BAV is normally inherited.

Aneurysm of the aortic sinus, also known as the sinus of Valsalva, is a rare abnormality of the aorta, the largest artery in the body. The aorta normally has three small pouches that sit directly above the aortic valve, and an aneurysm of one of these sinuses is a thin-walled swelling. Aneurysms may affect the right (65–85%), non-coronary (10–30%), or rarely the left coronary sinus. These aneurysms may not cause any symptoms but if large can cause shortness of breath, palpitations or blackouts. Aortic sinus aneurysms can burst or rupture into adjacent cardiac chambers, which can lead to heart failure if untreated.

A thoracic aortic aneurysm is an aortic aneurysm that presents primarily in the thorax.
An aortic sinus, also known as a sinus of Valsalva, is one of the anatomic dilations of the ascending aorta, which occurs just above the aortic valve. These widenings are between the wall of the aorta and each of the three cusps of the aortic valve.
A transthoracic echocardiogram (TTE) is the most common type of echocardiogram, which is a still or moving image of the internal parts of the heart using ultrasound. In this case, the probe is placed on the chest or abdomen of the subject to get various views of the heart. It is used as a non-invasive assessment of the overall health of the heart, including a patient's heart valves and degree of heart muscle contraction. The images are displayed on a monitor for real-time viewing and then recorded.

In human anatomy, the bronchial arteries supply the lungs with oxygenated blood, and nutrition. Although there is much variation, there are usually two bronchial arteries that run to the left lung, and one to the right lung, and are a vital part of the respiratory system.

The thoracic aorta is a part of the aorta located in the thorax. It is a continuation of the aortic arch. It is located within the posterior mediastinal cavity, but frequently bulges into the left pleural cavity. The descending thoracic aorta begins at the lower border of the fourth thoracic vertebra and ends in front of the lower border of the twelfth thoracic vertebra, at the aortic hiatus in the diaphragm where it becomes the abdominal aorta.
The aortic arch, arch of the aorta, or transverse aortic arch is the part of the aorta between the ascending and descending aorta. The arch travels backward, so that it ultimately runs to the left of the trachea.

Arterial switch operation (ASO) or arterial switch, is an open heart surgical procedure used to correct dextro-transposition of the great arteries (d-TGA).
The Ross procedure, also known as pulmonary autograft, is a heart valve replacement operation to treat severe aortic valve disease, such as in children and young adults with a bicuspid aortic valve. It involves removing the diseased aortic valve, situated at the exit of the left side of the heart, and replacing it with the person's own healthy pulmonary valve (autograft), removed from the exit of the heart's right side. To reconstruct the right-sided exit, a pulmonary valve from a cadaver (homograft), or a stentless xenograft, is used to replace the removed pulmonary valve. Compared to a mechanical valve replacement, it avoids the requirement for thinning the blood, has favourable blood flow dynamics, allows growth of the valve with growth of the child and has less risk of endocarditis.
Annuloaortic ectasia is characterized by pure aortic valve regurgitation and aneurysmal dilatation of the ascending aorta. Men are more likely than women to develop idiopathic annuloaortic ectasia, which usually manifests in the fourth or sixth decades of life. Additional factors that contribute to this condition include osteogenesis imperfecta, inflammatory aortic diseases, intrinsic valve disease, Loeys-Dietz syndrome, Marfan syndrome, and operated congenital heart disease.
The following outline is provided as an overview of and topical guide to cardiology, the branch of medicine dealing with disorders of the human heart. The field includes medical diagnosis and treatment of congenital heart defects, coronary artery disease, heart failure, valvular heart disease and electrophysiology. Physicians who specialize in cardiology are called cardiologists.

Familial aortic dissection or FAD refers to the splitting of the wall of the aorta in either the arch, ascending or descending portions. FAD is thought to be passed down as an autosomal dominant disease and once inherited will result in dissection of the aorta, and dissecting aneurysm of the aorta, or rarely aortic or arterial dilation at a young age. Dissection refers to the actual tearing open of the aorta. However, the exact gene(s) involved has not yet been identified. It can occur in the absence of clinical features of Marfan syndrome and of systemic hypertension. Over time this weakness, along with systolic pressure, results in a tear in the aortic intima layer thus allowing blood to enter between the layers of tissue and cause further tearing. Eventually complete rupture of the aorta occurs and the pleural cavity fills with blood. Warning signs include chest pain, ischemia, and hemorrhaging in the chest cavity. This condition, unless found and treated early, usually results in death. Immediate surgery is the best treatment in most cases. FAD is not to be confused with PAU and IMH, both of which present in ways similar to that of familial aortic dissection.
The heart is a muscular organ situated in the mediastinum. It consists of four chambers, four valves, two main arteries, and the conduction system. The left and right sides of the heart have different functions: the right side receives de-oxygenated blood through the superior and inferior venae cavae and pumps blood to the lungs through the pulmonary artery, and the left side receives saturated blood from the lungs.











