SA’s COVID-19 Epidemic: Trends & Next steps
•
0 likes•1,909 views

The document below outlines efforts by the Department of Health to further help spread the curb of the coronavirus in South Africa.
























SA’s COVID-19 Epidemic: Trends & Next steps
- 1. SA’s Covid-19 epidemic: Trends & Next steps Prepared on 13th April 2020 by Salim S. Abdool Karim, FRS Chair: Ministerial Advisory Group on Covid-19 Director: CAPRISA – Centre for the AIDS Program of Research in South Africa CAPRISA Professor in Global Health: Columbia University Adjunct Professor of Immunology and Infectious Diseases: Harvard University Adjunct Professor of Medicine: Cornell University Pro Vice-Chancellor (Research): University of KwaZulu-Natal Director: DSI-NRF Centre of Excellence in HIV Prevention Prepared for Minister of Health Zweli Mkhize
- 2. Outline Part 1: The Coronavirus epidemic • The Coronavirus epidemic in South Africa • Why is South Africa not on the expected Covid epidemic trajectory? • How much community transmission in SA? • Some future epidemic scenarios Part 2: South Africa’s Covid-19 response • Stages of the SA Covid-19 response • Next steps: Stopping small flames to reduce the risk of raging fires • Conclusion
- 3. Source: Nature 2020 The first million cases of Covid-19 Wuhan seafood market
- 4. Country level epidemic trajectories
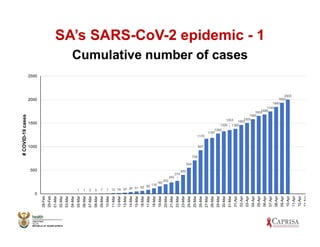
- 5. SA’s SARS-CoV-2 epidemic - 1 Cumulative number of cases 1 1 2 3 7 7 12 16 24 38 51 62 85 116 160 202 240 274 402 554 709 927 1170 1187 1280 1326 1353 1380 1462 1505 1585 16551686 1749 1845 1934 2003 0 500 1000 1500 2000 2500 28-Feb 29-Feb 01-Mar 02-Mar 03-Mar 04-Mar 05-Mar 06-Mar 07-Mar 08-Mar 09-Mar 10-Mar 11-Mar 12-Mar 13-Mar 14-Mar 15-Mar 16-Mar 17-Mar 18-Mar 19-Mar 20-Mar 21-Mar 22-Mar 23-Mar 24-Mar 25-Mar 26-Mar 27-Mar 28-Mar 29-Mar 30-Mar 31-Mar 01-Apr 02-Apr 03-Apr 04-Apr 05-Apr 06-Apr 07-Apr 08-Apr 09-Apr 10-Apr 11-Apr 12-Apr 13-Apr #COVID-19cases
- 6. 0 500 1000 1500 2000 2500 3000 3500 4000 19-Feb 29-Feb 10-Mar 20-Mar 30-Mar 09-Apr #COVID-19cases SA’s SARS-CoV-2 epidemic - 2 Trends in cumulative cases
- 7. SA’s SARS-CoV-2 epidemic - 3 Trends in new cases 0 50 100 150 200 250 300 05-Mar 06-Mar 07-Mar 08-Mar 09-Mar 10-Mar 11-Mar 12-Mar 13-Mar 14-Mar 15-Mar 16-Mar 17-Mar 18-Mar 19-Mar 20-Mar 21-Mar 22-Mar 23-Mar 24-Mar 25-Mar 26-Mar 27-Mar 28-Mar 29-Mar 30-Mar 31-Mar 01-Apr 02-Apr 03-Apr 04-Apr 05-Apr 06-Apr 07-Apr 08-Apr 09-Apr 10-Apr COVID-19cases Absolute number cases Moving average
- 8. Outline Part 1: The Coronavirus epidemic • The Coronavirus epidemic in South Africa • Why is South Africa not on the expected Covid epidenic trajectory? • How much community transmission in SA? • Some future epidemic scenarios Part 2: South Africa’s Covid-19 response • Stages of the SA Covid-19 response • Next steps: Stopping small flames to reduce the risk of raging fires • Conclusion
- 9. Covid-19 cases - SA vs UK SA’s expected vs actual trajectory Source: Tulio de Oliveira & UKZN CoV Big Data Consortium
- 10. SA’s epidemic trajectory is unique… Diagram source: Tulio De’ Oliviera & KZN CoV Big Data Consortium Why is SA different - new cases declining to a plateau: • Are we missing cases due to low or declining testing coverage? • Are there missing cases in poor communities due to skewed higher private lab testing? • Is the reduction genuine and due to the interventions in SA’s Covid-19 response?
- 11. Trends in cumulative private & NHLS Covid-19 tests show steady increase 0 200 400 600 800 1 000 1 200 1 400 2020-01-31 2020-02-06 2020-02-11 2020-02-14 2020-02-19 2020-02-25 2020-02-28 2020-03-03 2020-03-06 2020-03-09 2020-03-12 2020-03-15 2020-03-18 2020-03-21 2020-03-24 2020-03-27 2020-03-30 2020-04-02 2020-04-05 2020-04-08 Total Number of Tests Per Day Covid-19 cases have declined in the last 2 weeks while NHLS test numbers increased ie. while testing in people and communities without medical aid increased Note: Overall testing is still below the target of 10-15,000 / day
- 12. Outline Part 1: The Coronavirus epidemic • The Coronavirus epidemic in South Africa • Why is SA not on the expected trajectory? • How much community transmission in SA? • Some future epidemic scenarios Part 2: South Africa’s Covid-19 response • Stages of the SA Covid-19 response • Next steps: Stopping small flames to reduce the risk of raging fires • Conclusion
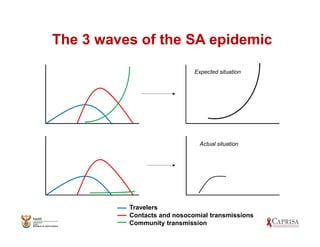
- 13. The 3 waves of the SA epidemic Travelers Contacts and nosocomial transmissions Community transmission Expected situation Actual situation
- 14. Why did SA not follow the expected epidemic curve? • First & second waves did not bridge spread effectively into the general community • No exponential increase in cases • If Ro > 1 daily average cases each fortnight/week would go up • Infectiousness is ~2 weeks - fortnight average of 65 cases/day before and 72 cases/day after lockdown suggests Ro ~1 around lockdown (Note: all cases are infections before lockdown) • No evident national increases in acute respiratory distress (may have some pockets) • If community transmission is low, cases decline • If community transmission is increasing then cases will increase and exponential curve will start again
- 15. Where is the highest risk of community transmissions in SA?
- 16. Outline Part 1: The Coronavirus epidemic • The Coronavirus epidemic in South Africa • Why is SA not on the expected trajectory? • How much community transmission in SA? • Some future epidemic scenarios Part 2: South Africa’s Covid-19 response • Stages of the SA Covid-19 response • Next steps: Stopping small flames to reduce the risk of raging fires • Conclusion
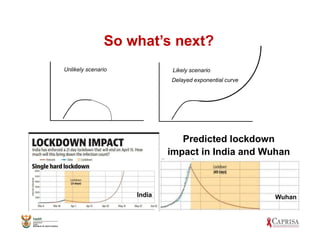
- 17. So what’s next? Delayed exponential curve Unlikely scenario Likely scenario Wuhan Predicted lockdown impact in India and Wuhan India
- 18. A difficult truth… Can SA escape the worst of this epidemic? Is exponential spread avoidable? • No! Not unless SA has a special protective factor (mojo) not present anywhere else in the world • Our population will be at high risk again after the lockdown • Infectiousness period includes 4-7 days before symptoms ie. people can spread it without knowing • The virus spreads too fast normally • Government interventions have slowed viral spread, the curve has been impacted and we have gained some time
- 19. Why the delay is important? • Time to flatten the curve even more • South Africa has a unique component to its response, ie. active case finding • Only South Africa has >28,000 community health care workers going house-to-house in vulnerable community for screening & testing to find cases • New quicker and simpler diagnostics becoming available • New treatments become available • Time to prepare for the medical care needs
- 20. Outline Part 1: The Coronavirus epidemic • The Coronavirus epidemic in South Africa • Why is SA not on the expected trajectory? • How much community transmission in SA? • Some future epidemic scenarios Part 2: South Africa’s Covid-19 response • Stages of the SA Covid-19 response • Next steps: Stopping small flames to reduce the risk of raging fires • Conclusion
- 21. Current stages of SA’s response Stage 1: Preparation • Community education • Establishing lab capacity • Surveillance Stage 2: Primary prevention • Social distancing & hand-washing • Closing schools and reduced gathering • Close the borders to international travel Stage 3: Lockdown • Intensifying curtailment of human interaction Stage 4: Surveillance & active case-finding • The Community response: door-to-door screening, testing, isolation and contact tracing
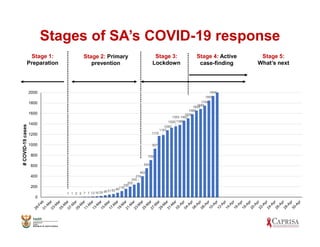
- 22. Stages of SA’s COVID-19 response Stage 1: Preparation Stage 2: Primary prevention Stage 3: Lockdown Stage 4: Active case-finding Stage 5: What’s next 1 1 2 3 7 7 12 16 24 38 51 62 85 116 160 202 240 274 402 554 709 927 1170 1187 1280 1326 1353 1380 1462 1505 1585 1655 1686 1749 1845 1934 0 200 400 600 800 1000 1200 1400 1600 1800 2000 #COVID-19cases
- 23. What should we do this week? Follow the lockdown rules and monitor community transmission by average daily cases & community positivity/screened 2 21 110 76 67 0 20 40 60 80 100 120 140 160 06 Mar - 12 Mar 13 Mar - 19 Mar 20 Mar - 26 Mar 27 Mar - 02 Apr 03 Apr - 09 Apr AveeragenumberCOVID019casesper week State of Disaster Lockdown Average daily Covid-19 cases last week = 67 (95% Confidence interval: 45-89) Next week? 10 Apr – 16 Apr
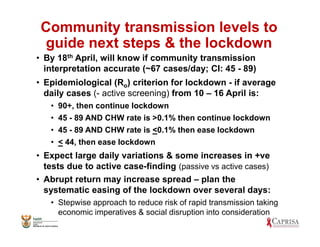
- 24. Community transmission levels to guide next steps & the lockdown • By 18th April, will know if community transmission interpretation accurate (~67 cases/day; CI: 45 - 89) • Epidemiological (Ro) criterion for lockdown - if average daily cases (- active screening) from 10 – 16 April is: • 90+, then continue lockdown • 45 - 89 AND CHW rate is >0.1% then continue lockdown • 45 - 89 AND CHW rate is <0.1% then ease lockdown • < 44, then ease lockdown • Expect large daily variations & some increases in +ve tests due to active case-finding (passive vs active cases) • Abrupt return may increase spread – plan the systematic easing of the lockdown over several days: • Stepwise approach to reduce risk of rapid transmission taking economic imperatives & social disruption into consideration
- 25. Next stages of South Africa’s response Stage 5: Hotspots • Surveillance to identify & intervene in hotspots • Spatial monitoring of new cases • Outbreak investigation & intervention teams Stage 6: Medical Care (for the peak) • Surveillance on case load & capacity • Managing staff exposures and infections • Building field hospitals for triage • Expand ICU bed and ventilator numbers Stage 7: Bereavement & the Aftermath • Expanding burial capacity • Regulations on funerals • Managing psychological and social impact Stage 8: Ongoing Vigilance • Monitoring Ab levels • Administer vaccines, if available • Ongoing surveillance for new cases Field hospital in Central Park, New York
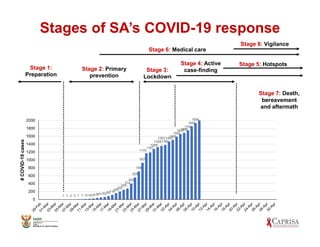
- 26. Stage 1: Preparation Stage 2: Primary prevention Stage 3: Lockdown Stage 4: Active case-finding Stage 5: Hotspots 1 1 2 3 7 7 12162438516285116 160 202 240 274 402 554 709 927 1170 1187 1280 1326 1353 1380 1462 1505 1585 16551686 1749 1845 1934 0 200 400 600 800 1000 1200 1400 1600 1800 2000 #COVID-19cases Stages of SA’s COVID-19 response Stage 6: Medical care Stage 8: Vigilance Stage 7: Death, bereavement and aftermath
- 27. Outline Part 1: The Coronavirus epidemic • The Coronavirus epidemic in South Africa • Why is SA not on the expected trajectory? • How much community transmission in SA? • Some future epidemic scenarios Part 2: South Africa’s Covid-19 response • Stages of the SA Covid-19 response • Next steps: Stopping small flames to reduce the risk of raging fires • Conclusion
- 31. Stage 8: Vigilance / surveillance • Need to stay one step ahead of viral spread and not wait for patients to arrive in hospitals to act • 3 components to surveillance: • Ongoing CHW house-to-house screening and testing especially in vulnerable communities • One day each month – health worker surveillance • One day each month - National surveillance day for schools, mines, prisons & big companies • For now self-taken swabs (later change to fingerprick) from a small sample of people in each setting
- 32. Major concerns for stage 6 – The medical care response • Poor health care access = ↑ deaths (NY) • Need an effective ambulance system • HIV+ (not on ART) & TB patients may ↑ severity • Both Covid & Flu epidemics intermingled • Need a voluntary partial lockdown until end September just for old people (>70 or >60) and those with co-morbidities to reduce exposure • Field hospitals for triage, mainly in big cities • Getting staff ready for the exponential curve, hospitals with makeshift ICUs, more ventilators & PPE
- 33. Conclusions • SA has a unique epidemic trajectory • Current trajectory due to curtailed community transmission from effective early interventions • The exponential curve is almost inevitable • Lockdown bought SA some time (about 4 to 6 weeks) and will likely reduce peak case load (flattened curve) • Systematic approach to keeping infection rates low while easing lockdown in stages • Focus shifts to Stage 5 of hotspot identification and intervention (fighting flames before they become fires), to Stage 6 – preparing for peak medical care response & Stage 8 – Vigilance & national surveillance
- 34. Acknowledgements Minister Zweli Mkhize & Professor Abdool Karim thank: • Nonhlanhla Yende-Zuma, Quarraisha Abdool Karim & Cheryl Baxter of CAPRISA • Tulio D’Oliviera of KRISP & KZN Big Data CoV Consortium • Yogan Pillay & Anban Pillay of the NDoH • Jane, Janine and Amanda of the secretariat • NatJoints Committee members • The Ministerial Advisory Committee for Covid-19 • The National Covid Command Council • All the hard-working people tackling the Coronavirus epidemic, especially health care workers on the frontline