Biomechanics and Treatment Planning - Part 1
•
11 likes•8,792 views

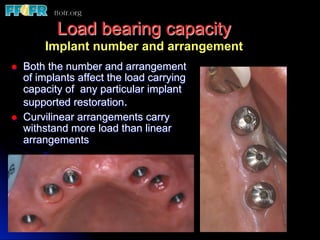
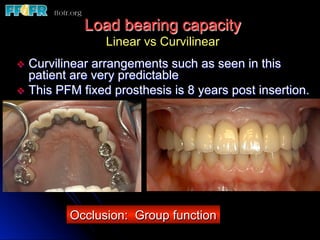
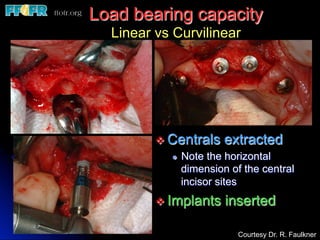
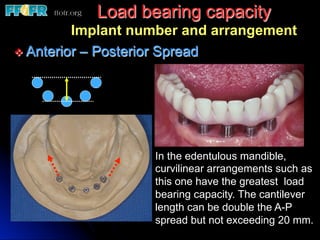
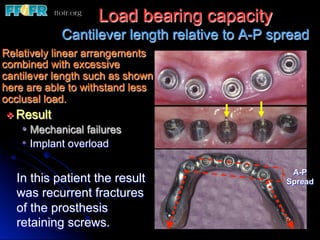
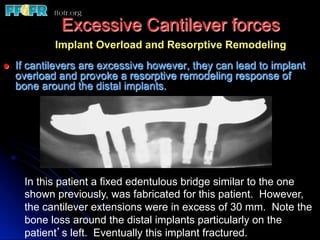
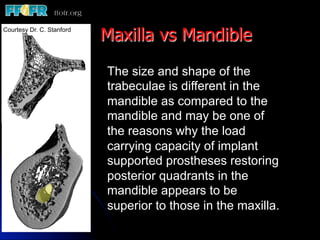
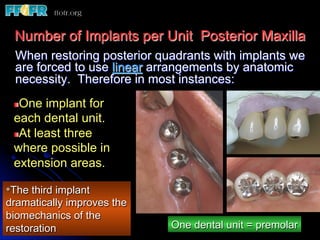
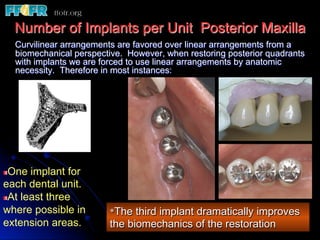
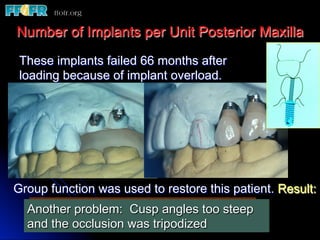
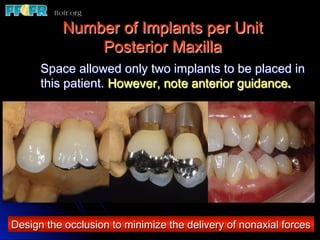
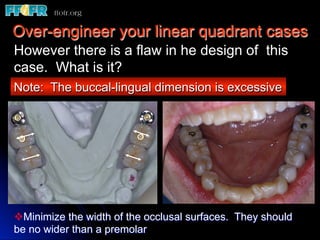
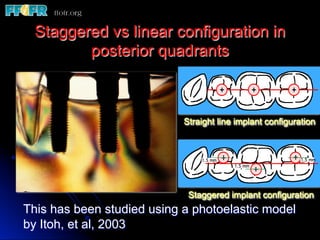
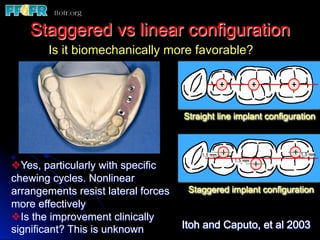
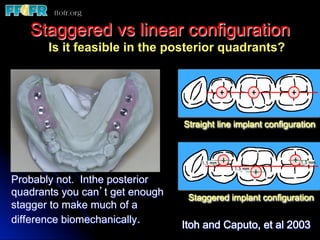
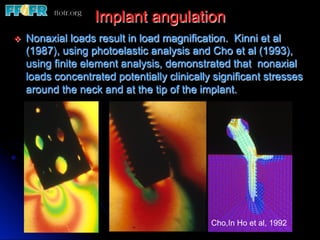
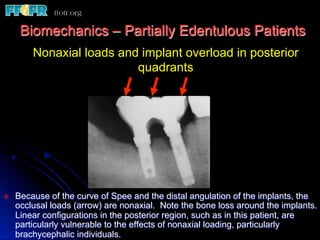
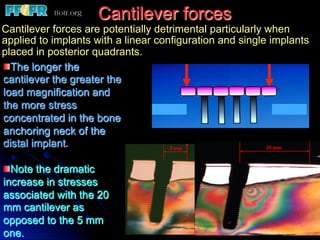
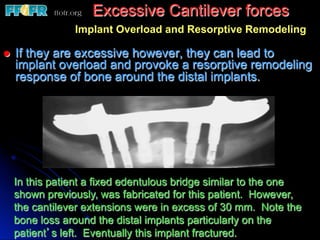
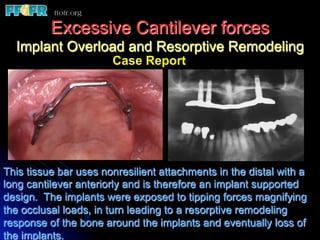
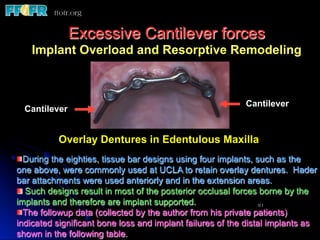
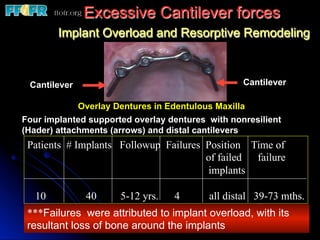
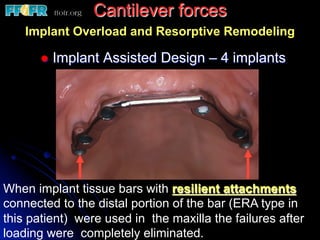
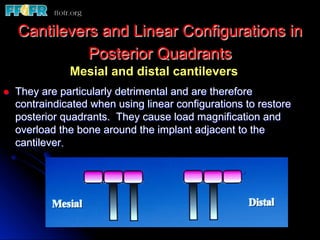
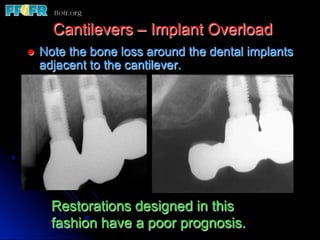
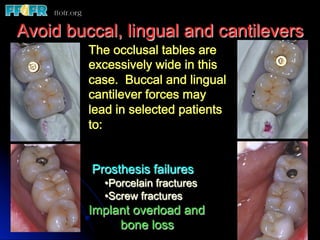
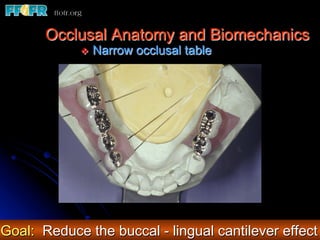
This document discusses implant biomechanics and treatment planning. It notes that implant overload can lead to bone loss and failure if excessive loads are placed on implants during treatment planning. Linear implant arrangements are less predictable than curvilinear arrangements, especially in posterior areas with heavy biting forces. The number of implants, their arrangement, angulation, length, diameter and the quality of surrounding bone all influence the load bearing capacity of implant restorations. Treatment plans must be designed to minimize non-axial forces and prevent implant overload.
1 of 81














Recommended
Implant occlusion
Implant occlusionDr Garima Singh Dental implants require different biomechanical considerations from natural teeth. Also, with one of the criteria for long-term implant success being “occlusion,” it becomes imperative for the clinician to be well
versed with the different concepts when rehabilitating with an implant prosthesis.
IMPLANT OCCLUSION
IMPLANT OCCLUSIONshari kurup This document discusses occlusal schemes for implants, known as implant protective occlusion (IPO). IPO aims to reduce stress at the implant-bone interface through 14 considerations including eliminating premature contacts, positioning occlusal contacts over implant bodies, reducing cantilever lengths, and decreasing crown heights. The goals of IPO are to reduce force magnification, improve force direction, and increase the implant support area to promote implant longevity and success.
Scientific rationale and biomechanics in implants
Scientific rationale and biomechanics in implantsMurtaza Kaderi This document discusses the scientific rationale and biomechanics related to dental implants. It defines biomechanics as the relationship between biological behavior of oral structures and the physical influences of dental restorations. The document outlines different types of biomechanics and discusses various biomechanical concepts including forces, stresses, strains and how these impact dental implants and surrounding bone tissue. It also examines factors that influence loading on implants like force magnitude, direction, duration and position in the dental arch.
Implant supported overdenture
Implant supported overdentureJISSA SUNNY This document provides an overview of implant supported overdentures. It defines overdentures and discusses the advantages and disadvantages compared to fixed prostheses. It describes different prosthetic options and classifications of prosthesis movement. Treatment options for mandibular and maxillary overdentures using various numbers and positions of implants are outlined. The focus is on removable prostheses that are partially retained by and supported by dental implants.
Biomechanics of RPD
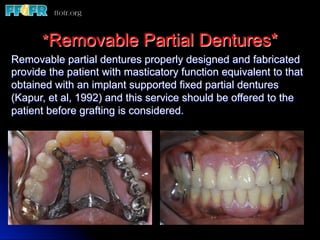
Biomechanics of RPDpadmini rani This document discusses the biomechanics of removable partial dentures. It begins by defining biomechanics in prosthodontics as the application of mechanical principles to biological tissues to design a stable prosthesis. It then discusses various types of stresses acting on partial dentures, including vertical, horizontal, and torsional stresses. Key biomechanical considerations for partial denture design are the length of the edentulous span, quality of ridge support, clasp design, and occlusal harmony. The document also covers biomechanical principles such as the snowshoe principle, L-beam effect, and concepts of levers, inclined planes, and rotation. The goal is to understand how to distribute forces across tissues to maximize prosthesis stability
Attachments in implant retained overdentures/ cosmetic dentistry training
Attachments in implant retained overdentures/ cosmetic dentistry trainingIndian dental academy Indian Dental Academy: will be one of the most relevant and exciting
training center with best faculty and flexible training programs
for dental professionals who wish to advance in their dental
practice,Offers certified courses in Dental
implants,Orthodontics,Endodontics,Cosmetic Dentistry, Prosthetic
Dentistry, Periodontics and General Dentistry.
Loading protocols in implant
Loading protocols in implantPiyaliBhattacharya10 loading protocols in dental implants about indications and contraindications of conventional , immediate,progressive and delayed loading of dental implants
Biomechanics dental implants
Biomechanics dental implantsMohamed M. Abdul-Monem This document discusses the biomechanics of dental implants. It explains that osseointegration is the direct bonding of bone to implant surfaces. Studying biomechanics is important because implants must withstand stresses from chewing forces. Implant failures can occur early during healing or later under loading. Failures result from overloading, infection or inadequate bone. Biomechanics applies engineering principles to dental problems. Forces during chewing create both vertical and horizontal stresses on implants. Key biomechanical factors for implants are inclination, preload, material properties, design, and surrounding bone quality and quantity.
Edentulous Maxilla - Fixed Prostheses
Edentulous Maxilla - Fixed Prostheseswww.ffofr.org - Foundation for Oral Facial Rehabilitiation This document discusses different treatment options for edentulous maxillas including fixed prostheses and implant supported/assisted prostheses. It covers patient selection factors like resorption patterns, jaw relations, lip line, sinus anatomy and economics. Minimum implant requirements, biomechanics, complications and different types of fixed prostheses like PFM and hybrid are described. The document also presents a clinical case of an implant supported fixed partial denture.
Centric relation
Centric relationBahjat Abuhamdan In prosthodontics, replacing the missing, without affecting the other components of the masticatory system has two main reference the maximum intercupation and the centric relation.
In this lecture discussion of centric relation as reference is exposed.
Occlusal splints
Occlusal splintspadmini rani An occlusal splint is a removable dental appliance that covers the biting surfaces of the teeth in one dental arch. There are several types of occlusal splints classified based on their design and intended use. The main types include permissive splints, non-permissive splints, and anterior repositioning splints. Occlusal splints are used to treat temporomandibular joint disorders by relaxing the jaw muscles, supporting the jaw in an optimal position, and reducing forces on the teeth and jaw joints.
Prosthetic management of tmd
Prosthetic management of tmdNishu Priya This document discusses various treatment methods for temporomandibular disorders (TMDs). It separates treatments into definitive treatments, which aim to eliminate the underlying cause, and supportive therapies, which aim to manage symptoms. Definitive treatments include reversible occlusal appliances, irreversible occlusal therapies, relaxation techniques, and management of parafunctional habits. Supportive therapies include medications, physical therapies like ultrasound and manual techniques, and self-care methods. The document provides detailed descriptions and indications for different appliance types, including stabilization, anterior repositioning, and soft splints.
Implant loading
Implant loading bhuvanesh4668 There are several protocols for loading dental implants after surgery based on bone density and healing time requirements. Protocols include Brånemark's loading protocol, progressive loading, and immediate/early loading. The density of the bone where the implant is placed determines the appropriate loading protocol, as less dense bone requires more healing time before loading to allow for sufficient bone mineralization and strength. Progressive loading gradually increases stress on the implant over time to allow the bone to adapt, reducing risks of failure. It is particularly important for lower density bone which is weaker.
Occlusion in implant ss
Occlusion in implant ssMurtaza Kaderi The document discusses occlusal considerations for implant-supported prostheses. It introduces various occlusal terminology and explores the significance of occlusion on osseointegrated implants. The document outlines the goals of implant protective occlusion (IPO), which aims to distribute occlusal forces appropriately to minimize stress on implants and surrounding bone. IPO principles include using thin articulating paper for initial adjustment, equalizing contacts under heavy bite forces, avoiding non-axial and offset loads, and designing the occlusion around the weakest component. The document also discusses factors like implant angulation, crown height, bone quality and the materials used for occlusal surfaces.
FULL MOUTH REHABILITATION
FULL MOUTH REHABILITATIONILA YADAV This document provides an overview of full mouth rehabilitation. It defines full mouth rehabilitation according to GPT-8 as restoring the form and function of the masticatory apparatus as nearly normal as possible. It discusses the objectives and indications for full mouth rehabilitation. It classifies full mouth rehabilitation into three categories based on the degree of wear and available space. It reviews different occlusal approaches, schemes, concepts and philosophies for full mouth rehabilitation including balanced articulation, group function and mutually protected articulation. It also discusses Hobo's twin table and twin stage techniques.
01 facebows and Articulators
01 facebows and ArticulatorsAmal Kaddah The document discusses facebows, which are dental devices used to relate the maxillary arch to the axis of rotation of the temporomandibular joint. There are two main types: mandibular facebows, which locate the exact hinge axis, and maxillary facebows, which relate the maxilla to the hinge axis position and transfer this to the articulator. The facebow registration is important for duplicating jaw movements on the articulator and accurately mounting dental casts. The document describes the components, use, and landmarks of facebows.
Neutral zone technique Journal club presentation
Neutral zone technique Journal club presentationDr Mujtaba Ashraf The document summarizes the neutral zone impression technique for constructing complete dentures. It describes the neutral zone as the area where the forces of the tongue pressing outwards are balanced by the forces of the cheeks and lips pressing inwards. The technique involves making an impression of the neutral zone using a tissue conditioner material while the patient performs functions like swallowing and talking to determine the optimal denture position and shape. This impression is then used by the dental technician to construct a wax denture try-in that precisely follows the contours of the neutral zone.
Biomechanics in implantology
Biomechanics in implantologyAnuja Gunjal This document discusses biomechanics as it relates to implantology. It defines key biomechanical concepts such as force, stress, strain and their relationships. Forces on dental implants can come from biting or parafunctional habits and are made up of compressive, tensile and shear components. The magnitude of stress on implants is determined by the applied force and the cross-sectional area over which it is distributed. Maintaining low stress levels is important for long-term implant success and minimizing risk of failure. Biting forces on natural teeth can range from 100-2400 Newtons and impact loads present additional risk. Biomechanical principles guide optimal implant design and placement to ensure forces are properly dissipated.
Occlusal equilibration - Kelly
Occlusal equilibration - KellyKelly Norton This document discusses occlusal equilibration and selective grinding. It begins by defining the key characteristics of a stable occlusion and the signs of an unstable occlusion. It then outlines the principles, indications, goals and procedures for occlusal equilibration and selective grinding. Specific techniques are covered such as how to eliminate interferences in centric relation, achieve the centric contact position, and adjust for lateral and protrusive interferences. The document emphasizes developing simultaneous contacts between cusp tips and flat surfaces to achieve occlusal stability.
Implant abutment and implant abutment connections
Implant abutment and implant abutment connectionsDR.BHAVESH JHA this ppt enlightened with different types of implant abutment connection. Detailed classification of abutments. Different types of abutments. Latest trends of abutments. Smart abutments. Platform switching, rationale of platform switching and related articles.
Full mouth dawson
Full mouth dawsonAnish Amin This document discusses concepts and techniques related to occlusal rehabilitation. It covers topics such as centric relation, anterior guidance, restoring anterior and posterior teeth, and solving various occlusion problems. The Pankey-Mann-Schuyler philosophy advocates establishing stable centric stops, proper anterior guidance in harmony with jaw movements, disclusion of posterior teeth in protrusion, and non-interference of teeth during lateral excursions. The document provides guidelines for determining tooth contours and positions to achieve optimal function, stability, and aesthetics.
01 facebows
01 facebowsAmal Kaddah The document discusses facebows, which are dental devices used to relate the maxillary arch to the hinge axis of opening and closing. A mandibular facebow can locate the exact hinge axis by using condylar rods to determine the axis of rotation. A maxillary facebow relates the maxilla to this axis and transfers it to the articulator to allow for accurate mounting. It describes how facebows help duplicate opening/closing arcs and lateral jaw movements. Common landmarks and methods for arbitrary and exact hinge axis determination are also outlined.
Full mouth hobo
Full mouth hoboAnish Amin This document discusses the theoretical background and techniques of the Hobo full mouth rehabilitation approach. It defines key terms like condylar guidance, incisal guidance, and disocclusion. It explains that the goal of reorganizing occlusion is to address issues like trauma, poor function, or lack of space. The optimal occlusion balances factors like condylar path, incisal guidance, and cuspal angles. The articulator aims to replicate these concepts to guide reconstruction of the full mouth.
journal club presentation on prosthodontics
journal club presentation on prosthodonticsNAMITHA ANAND This study measured and compared the stress transmitted to implants from different attachments for mandibular implant overdentures. An edentulous mandibular model with implants in the canine regions was fabricated. Strain gauges attached to the implants measured stress under vertical pressure applied to the denture. A locator attachment transferred more stress to the working side implant than a bar/clip attachment. Stress on implants decreased as the denture base length was reduced. The bar/clip attachment distributed stress more evenly between working and non-working side implants.
Neutral zone in complete dentures
Neutral zone in complete denturesDR PAAVANA This document discusses the neutral zone in complete dentures. It defines the neutral zone as the area in the mouth where forces from the tongue pressing outward are balanced by forces from the cheeks and lips pressing inward. It describes the muscles involved and how their forces influence tooth position and denture stability. It also discusses how the edentulous mouth changes over time, increasing the importance of properly recording the neutral zone for complete denture fabrication.
Mandibular movements /cosmetic dentistry courses
Mandibular movements /cosmetic dentistry coursesIndian dental academy The Indian Dental Academy is the Leader in continuing dental education , training dentists in all aspects of dentistry and
offering a wide range of dental certified courses in different formats.for more details please visit
www.indiandentalacademy.com
All On Four Dental Implant System
All On Four Dental Implant SystemUS Dental It describes All on four dental implant system, its advantages & steps, Post operative care & live cases at US Dental.
3.implant components and basic techniques3
3.implant components and basic techniques3www.ffofr.org - Foundation for Oral Facial Rehabilitiation The document discusses various implant components including fixtures, abutments, gold cylinders, and analogs. It describes the original Brånemark implant design and newer implant systems with enhanced surfaces and internal connections. The document also outlines different types of abutments from healing abutments to custom UCLA abutments and discusses techniques for impression taking and creating prosthetics on implants.
Edentulous Mandible - Fixed Prostheses
Edentulous Mandible - Fixed Prostheseswww.ffofr.org - Foundation for Oral Facial Rehabilitiation This document discusses various considerations for treatment planning and prosthodontic rehabilitation of edentulous mandibles with dental implants. It covers factors such as biomechanics, esthetics, oral hygiene access, and amount of keratinized tissue. Minimum implant number, length, and spacing are outlined. Techniques for impressions, soft tissue grafting, and fixed prosthesis options like PFM and hybrid are described.
Angled implants
Angled implantswww.ffofr.org - Foundation for Oral Facial Rehabilitiation This document discusses dental implants, specifically angled (tilted) implants used to restore edentulous maxillas. It describes several approaches for using tilted implants, including placing 4-6 implants with angled abutments to offset the implant angles, or using co-axis implants where angulation correction is subgingival. Tilted implants provide advantages like longer distal implants, improved primary stability, and eliminating the need for sinus augmentation. Studies show success rates above 90% for tilted implants.