






While this is a phenomenon more often seen in patients who are on continuous therapy for > 48 hours ("NIPPV" for ventilatory failure), there are a number of factors involved:
Risk Factors for Pressure Ulcer Formation
• Old age
• Dehydration
• Hypotension
• Hypoxemia
• Anemia
• Diabetes
• Atherosclerosis
• Malnutrition
• Vitamin C Deficiency
• Corticosteroid use
Prevention is key. At the first sign of redness, do something. Change mask, moving to an interface such as nasal pillows or FitLife.
There is a progression of pressure ulcer severity, graded through Wound Staging:
Wound Staging Guide
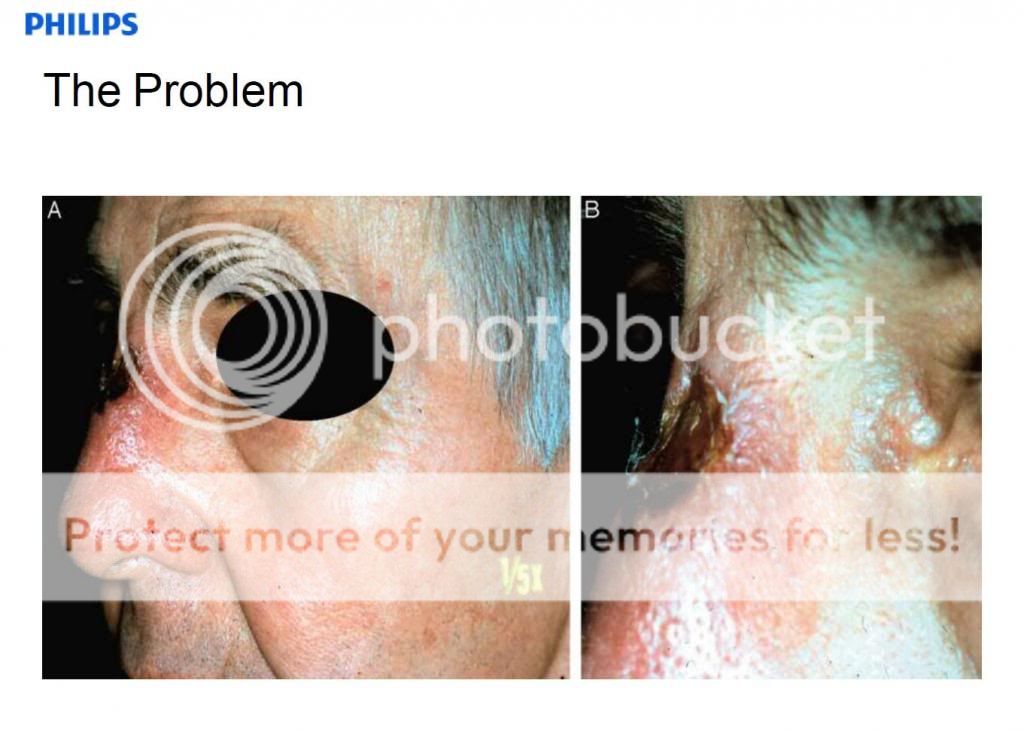
The key word is "blanching". Blanching is when you see an area of redness, press on it and remove your finger. If the tissue is white (ish) but returns to pink or red, that's "blanching". Persistent redness denotes non-blanchable tissue and a Stage 1 Pressure Ulcer. And here comes "The Big Deal":
The bridge of the nose is not only susceptible to pressure ulcers, but since there is a lack of adipose tissue, a Stage 1 ulcer, if allowed to progress, will usually jump to Stage 3 and beyond, and now you've got a HUGE problem.
Prevention strategies (if there's absolutely NO way to change your interface) include the use of barrier materials:
- REMzzz's
- Gecko
- High end approaches, such as 3M Barrier Wipe and Mepilex Dressing