

Abstract
Background:
Cross-institutional (external) referrals are prone to communication breakdowns, increasing patient safety risks, clinician burnout, and healthcare costs. To close these external referral loops, referring primary care physicians (PCPs) need to receive patient information from consultants at different healthcare institutions. Although existing studies investigated the early phases of external referral loops, we lack sufficient knowledge about the closing phases of these loops. This knowledge could allow health care institutions to improve care coordination and rates of closed referral loops by implementing socio-technical interventions for patient information exchange throughout a referral loop. Human factors engineering (HFE) provides a systematic approach to advance our understanding of barriers perceived by physicians. Using HFE, our objective was to characterize referring and consulting physicians’ barriers to closing referral loops and implications for care.
Methods:
This qualitative cross-sectional study included semi-structured interviews with referrers and external consultants. We used the Systems Engineering Initiative for Patient Safety 2.0 framework to conduct rapid qualitative analyses, determining perceived barriers and related implications. Main measures were consultants’ and referrers’ perceptions of, and experiences with, barriers to external referrals.
Results:
Six referring PCPs and 12 consultants participated from two healthcare systems and four medical specialties. Physicians perceived three main barriers in external referrals: receipt of excessive and unnecessary faxed documents, missing or delayed documentation, and organizational policies regarding information privacy interfering with closing the loop. Compared to internal referrals, physicians reported increased staff burden, patient frustration, and delays in diagnosis with external referrals. Consultants reported the ability to provide the same level of care to patients with internal or external referrals. However, consultants described communication breakdowns that prohibited confirmation of follow-up plan retrieval, initiation, or effectiveness.
Conclusion:
Physicians reported technological and organizational barriers to closing cross-institutional referral loops. Promises of HIE technology for external referrals have not fully materialized. Among physicians and patients, retrieval and exchange of medical information increases perceived workload, burden, and frustration. These increases are not accurately captured by traditional organizational metrics. This study provides evidence that informs future human factors engineering research to address perceived barriers and guide future HIE design or implementation.
Keywords: Consultation, Primary Care, Communication, Health Information Exchange, Usability
Introduction
By some reports, approximately 30%–50% of all outpatient specialty referrals are not completed successfully.1–4 As patients visit various clinicians, communication breakdowns can occur, increasing patient-safety risks, clinician burnout, healthcare costs, and malpractice claims.5, 6 For example, lack of timeliness and inadequate physician-to-physician communication may result in delayed diagnoses, threatening quality of care.7, 8 Specialty consultations involve complex processes of care coordination, requiring care transitions, information exchange, and physician communication (Figure 1). Generally, “closing the referral loop” means the referrals from a primary care physicians (PCP) or referrer to consultants result in completed specialty consultations, with results made available to referrers. 9 The US Centers for Medicare & Medicaid Services have identified closing the referral loop as a critical aspect in the referral process and acknowledge it as a national priority.3, 10
Figure 1. The referral process loop: the scope of closing the referral loop can include all of the blue boxes.
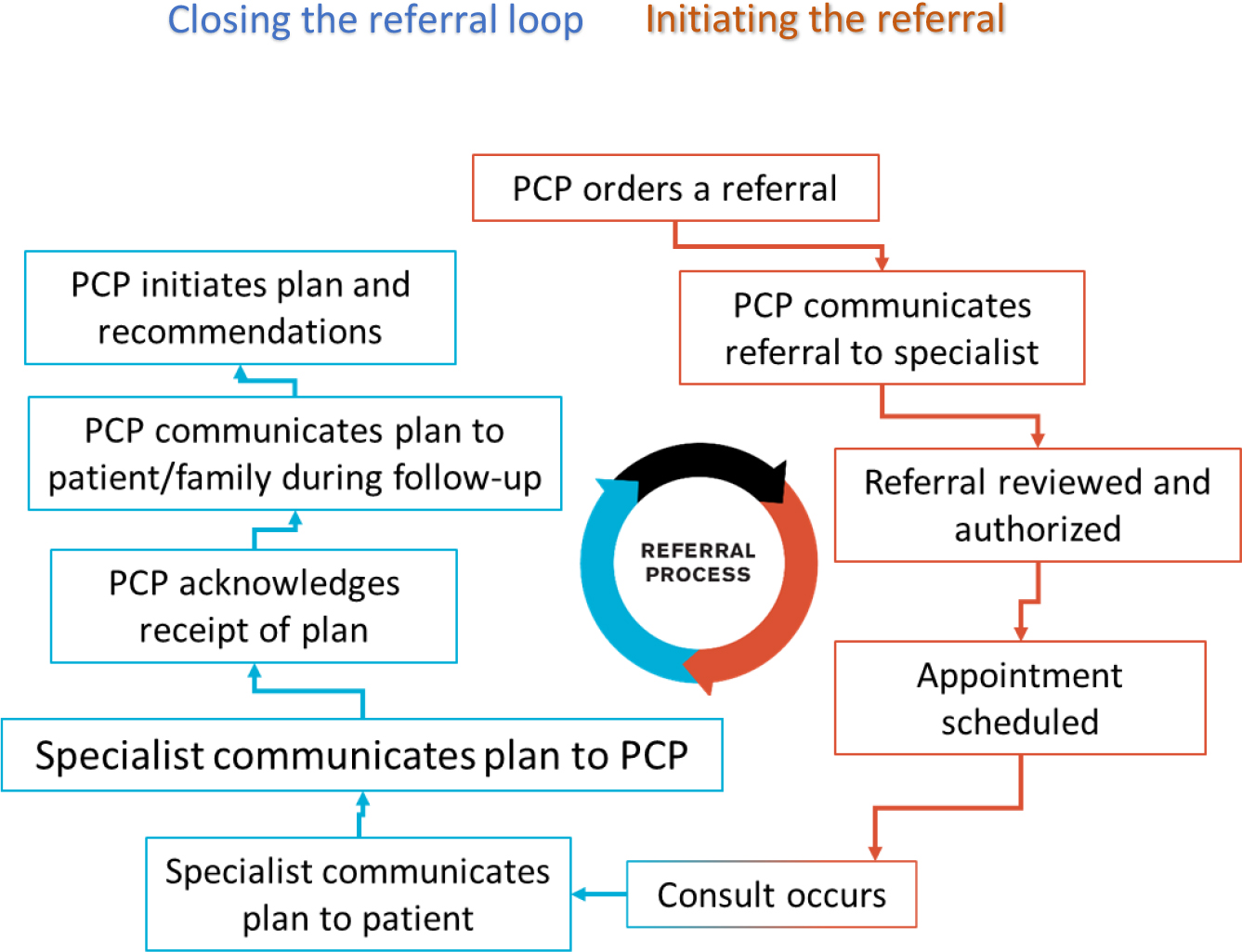
Adapted from Institute for Healthcare Improvement.11
Due to required information exchange across healthcare institutions, cross-institutional (external) specialty referrals are especially prone to inefficient workflows and communication breakdowns. To reduce these breakdowns and increase efficiency, technical advances in electronic health information exchange (HIE) standards and networks have been made. HIE software and technologies can enhance care coordination by aggregating and sharing patient information from multiple sources across healthcare institutions.12 For example, an HIE could present the consultant’s treatment plan to the referrer. However, low adoption rates, poor usability, and implementation issues with HIE technologies have limited their use and effectiveness. 9, 13–15 One cross-country study of HIEs denoted complications among physician communication during transfers of care and referrals.16 Results or plans received by referrers are commonly documents in various formats that contain untimely, irrelevant, conflicting, or incomplete information.9, 15 As a result, an estimated 10% of referrers’ clinic time is spent on referral management.17 Furthermore, referrers may have to make clinical decisions or initiate follow-up plans in spite of uncertainty and lack of trust in health information technology,13, 18–20 potentially negatively affecting clinical workflows 14, 21 or outcomes22, 23.
In contrast to research findings pertaining to referrers, fewer publications exist about consultants’ roles and experiences in closing cross-institutional referral loops. There is a need to improve the understanding of barriers perceived by consultants and their implications on clinical workflows. Physicians’ experiences have provided unique insights into clinical workflows and related processes.4, 15, 17, 24, 25 Referrers’ and consultants’ roles differ as their interactions vary among people, technology, and settings. A better understanding of consultants’ experiences is essential for identifying facilitators and barriers to closing cross-institutional referral loops during phases of the referral process that are often obscure to referrers. Consultants can provide unique insights into patient information quality and the communication of treatment plans to patients, caregivers, and referrers that could inform interventions to improve health information communication, decrease patient safety risks, and decrease clinician burnout. As the volume of cross-institutional specialty referrals increases,10, 15 the potential for communication breakdowns and risks to patients also increase.25
Using a human factors approach, our study’s objectives were to characterize consultants’ and referrers’ perceived barriers to completing external referrals, and those barriers’ implications for patient care. Human factors is a discipline combining engineering and behavioral science to study and improve work systems, comprised of interactions between people and their tasks, tools, and environments.26 Human factors engineering applies scientific methods, international standards, and established frameworks to identify problems and opportunities in those interactions, and to foster design and evaluation of evidence-based solutions. In healthcare, human factors engineering informs the design, evaluation, and implementation of human-centered information technology.27 Characterization of consultants’ and referrers’ perceived barriers through the lens of human factors engineering will help identify recommendations for enhancing the design and implementation of HIE technologies and their impact on care.
Methods
The Systems Engineering Initiative for Patient Safety (SEIPS) 2.0 framework guided semi-structured interviews with physicians.28–30 This human factors engineering framework consists of five work system factors—people, environment, tasks, tools, and organization—and their interactions, which can be used to describe how health care providers’ work systems affect workflows and outcomes.29 Interviews focused on scenarios, preferences, and barriers specific to the use of HIE and supporting technologies to close referral loops within (internal) and across (external) institutions. These interviews addressed two core domains: work system barriers to information sharing and communication, and implications for care.
Participants, Settings, and Recruitment
Physicians from primary care clinics and specialized consulting clinics at academic medical centers were targeted for recruitment, primarily from two healthcare networks in the Midwest. As a tax-supported, federally qualified health center, one of these networks serves vulnerable populations and uses EPIC’s electronic health record (EHR) system. The other healthcare network has the largest network of physicians in the state and uses Cerner’s EHR system. Both provide physicians access to HIE technology, such as CareWeb31 and Docs4Docs32. We sought to recruit at least 12 PCP referrers and 12 consultants to reach data saturation, which is typically reached with approximately 10–15 participants.33 We defined data saturation as the point at which no new data topics from participant interviews. We used convenience sampling for both groups, due to recruiting difficulties posed by the COVID-19 pandemic. PCPs from primary care and internal medicine were eligible for the referrer interviews. We targeted specialties with high numbers of referrals.34, 35 Consultants from neurology, gastroenterology, cardiology, and oncology were eligible. Our intent was to recruit at least three participants from each specialty. Contact information for potential participants was identified by key administrators and online directories. Eligible clinicians were contacted via email and phone calls.
Data Collection
We conducted semi-structured interviews with participating PCPs and specialty consultants. Interviews lasted up to 45 minutes and were conducted one-on-one virtually, using Zoom for Healthcare. Interview guides (see Appendix) were developed using the SEIPS 2.0 framework with questions emphasizing work system components related to internal and external referrals (Table 1). Questions focused on physicians’ needs and experiences in relation to their tasks, existing tools and technology, environment, and related policies. Interviews began with questions related to demographics, including each participant’s role, years of experience, and specialty. Two members of the research team (AS1, AS2, AM, EC, and AMG) were present for each interview; one served as the primary interviewer, and the other as a notetaker. All interviews were audio-recorded with participants’ consent and were transcribed for analysis.
Table 1.
Definitions of work system factors, and examples of characteristics in System Engineering Initiative for Patient Safety (SEIPS) 2.030
| Work System Factors | Definition | Examples |
|---|---|---|
| Tools & Technology | Objects that people use to do work or that assist people in doing work. | Electronic Health Records (EHR), fax machines |
| Organization | Structures external to a person (but often put in place by people) that organize time, space, resources, and activity. | How do organizational policies affect both internal and external referrals related communication or information sharing? • Are you familiar with communication and information sharing practices or policies at other medical centers, especially as they relate to cross-institutional physician-dyads (referrers and consultants)? •Has that influenced the workflow here? How? •Do you feel like you can try new things to improve your work processes? |
| Person(s) | Care provider or another employee of a healthcare institution performing a range of tasks. | Consultants, referrers, care team, office staff, patients |
| Tasks | Specific actions within larger work processes. | Requesting lab results from external providers, entering notes to EHR, following up with patient after referral |
| Environment | Environment includes internal and external environment. Internal referring to characteristics of the physical environment, room, or building. External referring to macro-level societal, economic, ecological, or policy factors outside an organization. |
Internal environment: Describe the environment where the referral process occurs. External environment: How do federal or insurance policies affect both internal and external consultations/referrals related communication or information sharing |
Data Analysis
Rapid qualitative data analysis 36 occurred with an iterative inductive approach, with codes being defined a priori from the interview guide, and revised during initial analysis to include emerging themes. Three researchers (AM, AMG, SK) independently read all transcripts prior to analysis to become familiar with the data and to assess the utility of the pre-established template. The team met to discuss assessments and refined a common understanding of the template. Each interview was summarized by four researchers (AM, AMG, SK, MH) into an episode profile template. Themes were identified iteratively through the data reduction process until the team reached a consensus. Episode profiles and themes were then reviewed and validated by the larger research team. We illustrated themes with respondent quotations. Two members of the team (SK, AM) created a matrix of barriers, system factors, and quotations.
Results
Participants
We interviewed six referring PCPs and 12 specialty consultants (Table 2). Referrers were predominantly female (83%) and White (66%), with work experience ranging from 10 to 32 years. Referrers practiced internal medicine (N=3), geriatrics (N=2), or primary care (N=1). Consultants were predominantly male (58%), White (58%) or Asian (33%), with experience ranging from 11 to 46 years. Consultants practiced in gastroenterology (N=4); neurology (N=5); cardiology (N=2); or oncology (N=1).
Table 2.
Participant demographics.
| Referrers | Consultants | |||
|---|---|---|---|---|
| Demographic | Number | % | Number | % |
|
| ||||
| Gender | ||||
| Male | 1 | 17% | 7 | 58% |
| Female | 5 | 83% | 5 | 42% |
|
| ||||
| Race | ||||
| White | 4 | 66% | 7 | 58% |
| Black | 0 | 0% | 1 | 8% |
| Asian | 1 | 17% | 3 | 25% |
| More than one Race | 1 | 17% | 1 | 8% |
|
| ||||
| Years of Experience (Total) | ||||
| 11–15 years | 4 | 66% | 3 | 25% |
| 16–20 years | 1 | 17% | 3 | 25% |
| < 20 years | 1 | 17% | 6 | 50% |
|
| ||||
| Years with Current Health System(s) | ||||
| 0–5 years | 1 | 17% | 2 | 17% |
| 6–10 years | 3 | 50% | 1 | 8% |
| 11–15 years | 1 | 17% | 2 | 17% |
| 16–20 years | 0 | 0% | 3 | 25% |
| < 20 years | 1 | 17% | 4 | 33% |
|
| ||||
| Specialty | ||||
| Primary Care | 1 | 17% | 0 | 0% |
| Internal Medicine | 3 | 50% | 0 | 0% |
| Geriatrics | 1 | 17% | 0 | 0% |
| Gastroenterology | 0 | 0% | 4 | 33% |
| Cardiology | 0 | 0% | 2 | 17% |
| Neurology (Adult & Pediatric) | 0 | 0% | 5 | 42% |
| Oncology | 0 | 0% | 1 | 8% |
| More than one Specialty | 1 | 17% | 0 | 0% |
Overview: Perceived work system barriers and negative outcomes for physicians and patients
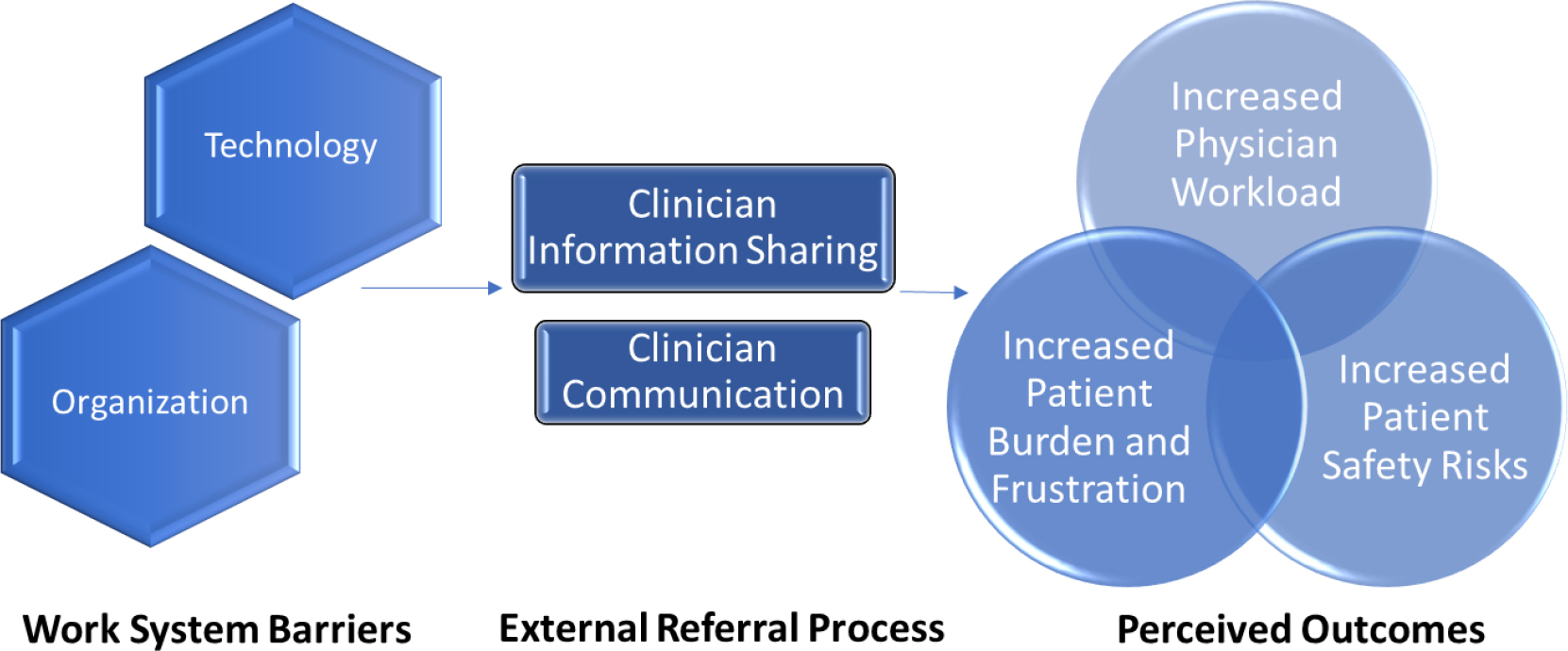
Based on our analysis using the SEIPS 2.0 model, technology and organizational factors were associated with the largest number of barriers. Person, task, and environment factors were not as prominent in the analysis of barriers. HIE technologies were described as “extremely difficult to navigate,” not user-friendly, and often containing errors and outdated or missing information. None of the participants reported integrating HIE technologies into their workflows. Overall, consultants perceived external referrals as being “a constant struggle for communication.” A consultant said, “I’m sure there are other avenues by which information should be shared, but you’ve got to deal with privacy and institutional policy and so forth. Bottom line, the better the information sharing is, the better the coordination of care and the smoothness of the delivery of care for the patient.” [Consultant 11] With current workflow and information flow challenges, referrers shared that they avoid making external referrals unless they are necessary (i.e., a required specialty not available in the referrer’s hospital system). The perceived barriers to closing the external referral loop were associated with perceived increases in patient safety risks, patient burden and frustration, and physician workload (Figure 2).
Figure 2. Findings applied to the SEIPS framework.
Technological barriers
When discussing barriers related to technology, information sharing and communication were hindered due to the use of rudimentary technology (see Table 3). Since communication and sharing of information occurred via fax and phone, consultants reported that it is “much harder” to communicate with referrers from other institutions. Consistent among consultants were descriptions of the “100-page fax,” detailing the frequent receipt of clinical information that was both excessive and unnecessary (i.e., included information not needed). Consultants also reported time wasted by trying to access information, only to discover that the desired information (labs, medications, etc.) was missing. Furthermore, consultants noted that they have no way of knowing whether the referrers ever receive their notes due to issues with outdated or missing contact information for referrers.
Table 3. Classification of perceived barriers to closing external referral loops by attributing work system factors.
Quotes included are representative for indicated participants (consultants or referrers).
| Work System Factor | Perceived Barrier | Participant Comment |
|---|---|---|
| Technology | Excessive and unnecessary information sent from referring physician – Fax machines | C: “Even when I have good records, a lot of times the referring providers … in an effort to be complete will send you 100 pages of records, and it can be all kinds of junk, you know. Like 100 pages that were not relevant.” [Consultant 1] |
| Technology | Outdated or missing contact information for physicians - EHR | C: “I don’t always know their address and those types of things, and usually the people who transcribe my notes are able to find it, but they are often more challenged finding those providers who are referring outside the health care system.” [Consultant 1] C: “That’s maybe a 70–30 bet. 70% of the time it’ll go okay; 30% of the time, … the system will tell you we can’t do that because we don’t have any contact info.” [Consultant 3] C: “Then for an external provider, let’s say that they were sent by Dr. John Smith. So, I go into my list of John Smiths in the electronic record to generate a letter to them. So how many John Smiths do you think are in it? And this has been a big, big problem for me.” [Consultant 11] |
| Technology | Exchange is based on rudimentary technology - Fax and phones | C: “Yeah, it’s [external referrals are] different and much harder. So, they [records] come by fax, they come by way of random emails, they come by phone call from the patient to a scheduling number.” [Consultant 4] C: “Traditionally, the fax referral is still the most common way we get them externally.” [Consultant 7] C: “The one aspect is whether I would potentially call the referring physician or not. That would probably be the one big difference.” [Consultant 12] R: “For external referrals, I don’t have any software that I’m using. It’s a script pad that I’m faxing.” [Referrer 2] |
| Technology | Missing or delayed documentation - EHR | C: “… Patients are frustrated. They had so many other things that were not sent over. Or, they had like 10 months’ worth of investigations, but I only got 10 pages from the last clinic visit. They go on to their phone and open chart review after chart review from the other hospital system, which can be very time-consuming.” [Consultant 2] C: “It’s not uncommon, unfortunately, that they get labs done that are supposed to get faxed to us, and they just get put in a pile and they don’t necessarily get faxed until the next day or the day after, or sometimes never get faxed.” [Consultant 12] R: “No, it’s a huge pain for external referrals because I can’t check to see if it’s been scheduled. I don’t know who to contact. And then even once they see the people there—I would say 80% of the time, I don’t know what’s been done. I don’t get any information back.” [Referrer 5] R: “But if it’s external and we’re not using the same EHR, sometimes I get a report, sometimes I don’t… sometimes I only have what the patient is telling me.” [Referrer 2] |
| Organization | Limiting organizational policies regarding information privacy | C: “HIPAA preventing sharing patient information via texting, which may be the only way to get into contact with a physician.” [Consultant 8] C: “The hospital system may or may not allow certain providers to have privileges at that hospital. And if they do, then their information on their patients is available through that hospital system. But there are some providers who don’t have privileges at the facility. And therefore, none of their patient information is in.” [Consultant 9] R: Very site-specific, regarding the Department of Veterans Affairs: “It’s now pretty difficult to sometimes share outside notes. To share our notes to the outside.” [Referrer 1] |
R - Referring primary care physician; C – Consultant
Organizational barriers
Organizational policies reportedly prevented information sharing and interpersonal communication between referrers and consultants from different institutions (Table 3). For example, referrers mentioned that external consulting institutions in need of information might have different policies and procedures about requirements for sharing or releasing their own information. Additional or unique requirements for consent forms were said to lead to communication breakdowns or delayed information sharing. According to consultants and referrers, some physicians’ privileges at multiple institutions helped to circumvent technical limitations for information sharing because they had access to multiple EHRs. However, this practice was not necessarily approved or considered to be an aspect of standard workflow.
Perceived increase in physician workload, patient burden, and patient safety risks
Attempting to access patient information, consultants perceived an increase in workload for both them and their teams. Consultants described repetitive phone calls to referrers’ clinics and testing sites to request information. Often, the information received was considered to be of poor quality regarding timeliness, relevance, and completeness. As a result, consultants noted that their workload increased after patient encounters. For instance, consultants described multiple phone calls to patients after a visit to discuss lab results that were not received prior to the consultation. Consultants said these phone calls were frequent and could last up to 20 or 30 minutes, sometimes resulting in a need to schedule another appointment. While these phone calls and additional appointments were perceived as an increase in workload, consultants mentioned that the extra time spent on phone calls is not recognized as a standard work metric (i.e., billable, reimbursable) by their organizations.
Consultants noted that communication breakdowns resulted in delayed patient care, and less time for the patient to receive direct care. Across specialties, consultants described scenarios in which patients were visibly burdened and frustrated (see Table 4). Providers perceived patients as disheartened to hear that not all of the necessary information was available to their physicians, delaying diagnosis or treatment. Without essential patient information, including all relevant labs, consultants relied on patients to recall past tests, medications, or clinical encounters. Consultants noted patients’ frustration as they attempted to find necessary information in folders of printouts or on mobile phones, which could dominate most of the encounter time. Additionally, patients would need to schedule yet another appointment, adding further stress and potentially redoing uncomfortable tests. Consultants noted that some patients wait a long time for an appointment or travel long distances, which is taxing on them and their caregivers. Furthermore, added stress could impact their medical conditions or symptoms.
Table 4. Classification of perceived outcomes related to perceived barriers.
Quotes included are representative for indicated participants (consultants or referrers).
| Perceived Outcome | Description | Work System Factor | Participant Comment |
|---|---|---|---|
| Increased physician workload | Increased information searching and coordination efforts | Organization and People | C: “Patients, who live far away or need appointments with multiple specialists require more effort. …We’ll have to coordinate if they need to see us and see ophthalmology or see cardiology, or they need a test done, trying to get all that testing done in a single visit. So, it falls on our staff who generally do a very good job of trying to coordinate those things, which is on short notice if they need to be done quickly.” [Consultant 7] C: “Wow, I spent 20 minutes looking for a test that isn’t even in here or a note that’s not even here.…I had to actually call that doctor’s office while the patient was in the room and get some records faxed, that’s the quickest way to get records. I reviewed records while the patient was there. Then, I talked to and examined the patient. Then, I called the doctor back. Typically, you’re spending maybe in this case, maybe 15 to 20 minutes physically with the patient and really spending time with them. But the whole process might have taken over an hour. …Most of that is spent on logistics, getting records, talking to other people, which is important. But you get an idea of sort of the magnitude of some of the inefficiencies that are built into the system.” [Consultant 3] C: “Additional visits don’t happen, but it does delay care because there are 10 other phone calls from maybe my assistant, my nurse. So, it’s a lot of manpower that goes into coordinating care between hospitals because there is no seamless system that is automatically happening.” [Consultant 2] |
| Increased patient burden | Less time with patient | Technology and Organization | C: “They’re holding a big manila envelope and I only have however long, 30 minutes to talk to them. Well now I’m going to be spending 20 of those minutes just flipping through a hundred pages… I like to spend time with the person, talking to them about their problem. I like going in already knowing all the data and then having them tell their story, and then we can talk about it. I don’t want to spend our time finding the data.” [Consultant 5] |
| Excess testing, retesting, appointments, and costs | Organization | C: “Patients are left with a feeling that they already spent so much money to get so many other tests. They’re not quite sure if it’s a good investment to get it retested…So, now you have two gastroenterologists taking care of one situation. And a lot of the testing that’s done at the outside place may not be sent to us.” [Consultant 2]C: “…nobody wants a $1,000 bill over a test that’s already been done. So, I think just diagnostic delays and incurred cost to patients when duplicate testing is done or kind of the things that concern me sometimes when patients come from outside.” [Consultant 3] R: “Starting the process over, or maybe doing something that’s inappropriate, especially with residents or patients with dementia, where it’s unreasonable that they could complete something, but they order it anyways—that’s frustrating.” [Referrer 2] |
|
| Over reliance on patients to transfer medical information | Organization and Technology | C: “Patients may experience anxiety when test results aren’t in their records since they were conducted externally.” [Consultant 2] C: “It’s their medical record, their doctor needs it. So, I’ll give it to them in person. Because sometimes they may not have the information, they don’t know who they might end up seeing or what the numbers are. And so, if it’s someone who has somewhat of a complicated story, say they are on some medicines that are important for them to continue, I will just do it on my end and give it to them.” [Consultant 8] |
|
| Increased patient safety risks | Poor clinician interpersonal communication | Organization | C: “There is a lot of communication no doubt that we communicate. But you cannot impose your recommendations on a different team because each hospital has its own culture, each team has its way of reacting to stuff.” [Consultant 2] C: “I’ll be frank with you, I often just re-consult somebody in our system. Sometimes I’ll reach out, but it’s like so hard to have any meaningful back and forth conversation. You try to call them and page them, they’re in clinic. They try to page you, you’re in clinic. You play phone tag like back and forth. There’s no way to kind of just email them. And so, a lot of times I’ll just say you [the patient] need to see one of our hematologists. Because I can’t, this is too big of a deal for me to trying to chase somebody down and we’re [me and your hematologist] need to be in constant communication about this blood thinner. With liver transplants, there’s a lot of care coordination, there’s a lot of stakeholders and we often end up re-consulting physicians that we can readily be in conversation with about their care. There’s few outside providers that I, end up talking to a lot.” [Consultant 1] R: “It just depends on that office and their protocol and their process. Some offices don’t seem to have a problem with the prompt response, and then some offices are really hard to get into.” [Referrer 2] |
| Delays in care | Technology and Organization | C: “I think the challenge oftentimes is, if coordinating the ability to give them a certain medication locally where they don’t have to travel too far to get here, making sure that there’s actually somebody who has the knowledge of those medications, so there’s certainly more rural areas of Indiana that may not have a hematologist readily available.” [Consultant 12] R: “When I order a consult, it’s not like this can be done in six months. You really want a fast answer, or you wouldn’t be ordering the consult if you could handle it yourself in two weeks. So, I think that the speed at which you achieve that consult is important. And I think there is a lot of care coordination in sharing why you feel they need to be seen quickly.” [Referrer 2] |
R - Referring primary care physician; C – Consultant
Although most consultants stated that external referrals present additional challenges, they also reported that aforementioned barriers did not necessarily affect patient safety (see Table 4). Given these barriers and challenges, referrers shared that they would encourage patients to stay “in the system” for all of their care, or to venture outside at their own risk. Both referrers and consultants indicated that the issue of communication and information sharing barriers did not contribute to medical errors or poor treatment. To the best of their knowledge, consultants stated that they were able to provide the same level of care to patients regardless of whether referral and consultation occurred at the same institution. However, some consultants reported they did not often know how patients’ health or safety was affected when the patient returned to the external referrer. Without clear communication or information sharing with the referrer, consultants explained that they would only become aware of patient issues, recommendation adherence, or need for additional treatment if the patient returned for another consultation.
Discussion
By applying SEIPS 2.0, we were able to systematically analyze physicians’ perceived barriers to closing external referral loops. Our human factors approach facilitated the identification of social and technical factors related to specialty care consultations across healthcare institutions and provided evidence to aid and enhance the understanding of physician-perceived barriers. Based on these perspectives, we discuss implications below.
Physician workload
Physicians said they felt a sense of “helplessness” and overload both professionally and personally, especially with respect to competing demands of clinical care and organizationally emphasized metrics (e.g., reimbursement). Our study described how misaligned organizational metrics and policies negatively affect physicians. Consultants described their institutions’ stance as closer to a business-centric approach to care, where the aim is to maximize patients and profits rather than emphasize meaningful experiences for patients and physicians. This phenomenon closely resembles emerging work37 characterizing physician burnout linked to EHR usage logs. In contrast, the use of rudimentary or inefficient technology such as telephones, fax machines, and printers does not generate the same types of usage data (e.g., time of logins, number of clicks, or page view duration) or workflow efficiency indicators. For example, time reviewing the “100-page fax” in addition to the EHR is not captured. The relative “invisibility” of such technologies in terms of logging, auditing, quality assessment, and research contributes to overlooked barriers. Our results indicate that this type of workload increase is experienced by the entire care team and is not limited to physicians.
Patient burden and frustration
When discussing their perceived barriers to closing external referral loops, physicians expressed concerns regarding patient burden, including increased information management, duplicate testing, delays in diagnosis, and patient frustration. Aligned with previous studies,15, 20 neither referrers nor consultants interviewed in this study trusted the successful transmission of clinical information via EHR or HIE technologies because of their firsthand experience with communication breakdowns. Our study described how physicians were forced to be over-reliant on patients to fill health information gaps during clinical encounters. Although physicians wanted to discuss undocumented information (e.g., goals, resources, new health concerns), the time required to search for missing medical data limited interpersonal discussions. The alternative option was duplicate testing, which is burdensome for patients due to costs, travel, discomfort, time required, and prolonged anxiety over results. Beyond delays to care access, our findings highlight the negative impacts of delayed access to patient information. Existing studies denote that reduced patient satisfaction or increased patient frustration affects health outcomes.38 Our findings indicate that HIE technology has fallen short of potential benefits, including duplicate testing regarding cross-institutional referrals. Across patient populations from varying backgrounds and with a variety of medical conditions, relying on patients’ access to and management of medical records to support referrals is not a robust solution and could introduce or exacerbate health disparities.
Patient Safety Risks
Although neither consultants nor referrers perceived great risks to patient safety or witnessed adverse outcomes from existing studies15, 23, both groups noted that communication barriers often limited or excluded knowledge or confirmation of patients’ health outcomes after external referrals. According to our interviewees, physicians’ privileges at multiple institutions helped to circumvent technical limitations for information sharing because they had access to multiple EHRs. However, usability and data quality issues are not limited to a specific EHR system.39 Therefore, access to multiple EHRs may not increase physicians’ awareness of patient safety risks.40 Regarding consent for release and electronic communication of medical records, both referrers and consultants reported inconsistencies among communication policies at different institutions limited interpersonal communication between the two groups. According to Singh et al.,41 limited follow-up and communication predisposes patients to diagnostic errors, degrading the evolution of diagnostic impressions.
Early recommendations and future research
Based on our results, the technology and organizational barriers perceived by physicians illustrated the necessity of communication and information sharing for patient care coordination across institutions. Consequently, potential for HIE technological solutions for cross-institutional referrals exists, but effective designs, implementation, and adoption are essential for future success. Applying a human factors approach, previous studies of newly designed, adopted, and implemented health information technology reported improvements in the referral process.17, 42, 43 This study provides evidence that informs future human factors research of HIE technology for closing external referral loops, emphasizing the human-centered design process (Box 1). Future research should investigate how emerging health information communication technology and applications (apps) can foster better interpersonal and medical record communication. For example, assessment of clinicians’ interactions via telephone and fax machines (e.g., time spent, number of attempts) can provide insights on extraneous efforts, essential information gaps, and reliable information sources. Existing literature describes design guidelines and use of electronic templates to improve referral orders.3, 44 For consultants, our evidence recommends applying HIE electronic templates or user interfaces accessible via EHRs, which can assist in transferring information from consultants to referrers. Extending the guidelines for data entry, we recommend customizable information displays that support filtering, sorting, and queries for additional information. This recommendation would address the perceived increased physician workload and patient burden invoked by relying on phone calls and faxes. Furthermore, we recommend salient feedback on these displays to confirm information receipt and post-consultation health outcomes. Future evaluation efforts to analyze health outcomes among internal and external referrals are needed to improve understanding of positive and negative associations, and implications for patient-safety risks.
Box 1. Early recommendations supported by results.
Recommendations
- Identify requirements for future technological and organizational interventions.
- Assess clinicians’ use of telephone and fax machines (e.g., time spent, number of attempts).
- Identify essential information gaps (e.g., lab tests, diagnosis, name of referrer).
- Identify reliable information sources.
- Design and evaluate HIE electronic templates or user interfaces prototype.
- Design customizable information displays; support filtering, sorting, and queries for additional information.
- Provide salient feedback to confirm information receipt and communication of post-consultation health outcomes.
- Assess usability of prototype, measuring efficiency, effectiveness, and satisfaction among referrers and consultants.
- Identify positive and negative associations among HIE technologies and closing cross-institutional referral loops or implications for patient-safety risks.
- Design clinical trials to analyze health outcomes among internal and external referrals.
*HIE – Health information exchange, EHR – electronic health record system.
Limitations
Due to the COVID-19 pandemic, this study was limited by a small convenient sample of interviewees in two healthcare facilities. However, one healthcare facility has the largest network of physicians in the state, and the other facility primarily cares for vulnerable populations. Although a small proportion of clinics within each facility were represented in this analysis, these specialties reported having large numbers of specialty referrals. Participants and non-participants may differ in their characteristics, practices, experiences, or perspectives. Further research in a representative sample is needed to confirm these results.
Conclusion
In this cross-institutional study, referring and consulting physicians reported technological and organizational barriers to closing cross-institutional referral loops. HIE technologies’ poor implementation, usability, and data quality deterred physician use and adoption. As a result, physicians’ information exchange and communication are over-reliant on patients and fax machines. In attempts (i.e., workarounds) to close cross-institutional referral loops, physicians described increases in workload, burden, and patient frustration, which were not accurately captured by routine organizational metrics. Considering the large demand for cross-institutional referrals, our findings indicate the need for a human factors approach to investigate and address sociotechnical barriers to closing cross-institutional referral loops.
Summary Table.
What was known:
Approximately 30%–50% of all outpatient specialty referrals are not completed successfully.
An estimated 10% of referrers’ clinic time is spent on referral management.
There is a need to improve understanding of barriers perceived by consultants and implications for clinical workflows and outcomes.
What this study added to our knowledge:
We characterize consultants’ and referrers’ perceived barriers to completing external referrals and implications for care.
Referring and consulting physicians reported technological and organizational barriers to closing cross-institutional referral loops.
In attempts to close cross-institutional referral loops, physicians described increases in workload, burden, and patient frustration, which were not accurately captured by routine organizational metrics.
Funders:
The research reported here was supported by Dr. Savoy’s early career development award, funded by the following grants KL2TR002530 and UL1TR002529 from the National Institutes of Health, National Center for Advancing Translational Sciences, Clinical and Translational Sciences Award. Drs. Savoy, Weiner, and Damush are supported by the U.S. Department of Veterans Affairs, Veterans Health Administration, Health Services Research and Development Service CIN 13–416. Dr. Weiner is Chief of Health Services Research and Development at the Richard L. Roudebush Veterans Affairs Medical Center in Indianapolis, Indiana. The views expressed in this article are those of the authors and do not necessarily represent the views of the U.S. Department of Veterans Affairs or the United States government. Teresa Damush PhD is supported by the VA HSR&D Research Career Scientist Award (IK6HX002715-03).
Abbreviations
- HIE
Health information exchange
- PCPs
Primary care physicians
- SEIPS
Systems Engineering Initiative for Patient Safety
- EHR
Electronic health record
Appendices
Appendix A: Referrer Interview Guide
This is an interview with [participant ID] on [date].
At which facility or facilities do you currently practice? How long have you worked at the [facility name]?
In what year did you receive the degree, such as M.D., that has enabled you to become a licensed health professional?
What is your job title?
Specialty?
Today we are here to learn from you about the differences between internal and external referral processes. During this interview, the internal referral process describes scenarios where both the referrer and consultant are in the same healthcare institution and use the same electronic health record system (EHR). An external or cross-institutional referral process describes scenarios where the referrer and consultant work in different healthcare institutions and do not use the same EHR. We would like to know how your workflow differs among these two scenarios, especially for the initial follow-up from consult. We would like to hear your perspective on provider communication, documentation, and workflow efficiency.
Characterize Workflow Differences
-
1
Describe your typical clinical workflow for ordering specialty referrals.
-
2How does your workflow differ if the referral is to external specialists?
- Are there the same number of steps/tasks or documentation for both scenarios?
- Describe any other software applications or communication processes that are used to support the referrals.
-
3Switching to your workflow after the consultation, please describe your workflow when following-up with patients after a specialty referral?
- What kind of information is needed to fully support your follow-up with a patient after a consultation (i.e., medication changes, diagnostic plan changes, specialist visit note)?
- What are the sources of information (e.g., care team, patients, consultant)?
- How do you retrieve information needed? What modes are used to share or communicate patient information (fax, phone calls, EHR, HIE – secure emails, etc.)?
-
4How does the workflow, information flow, or communication differ when patients have visited an external specialist/consultant?
- What kind of information is needed to fully support your follow-up with a patient after a consultation (i.e., medication changes, diagnostic plan changes, specialist visit note)?
- What are the sources of information (e.g., care team, patients, consultant)?
- How do you retrieve information needed? What modes are used to share or communicate patient information (fax, phone calls, EHR, HIE, secure messaging, etc.)?
- Do you have to use a system/software to access consultant notes from an external referral?
Clinical Example…
-
5Can you describe a case(s) where following an external consultation a patient required a high-level of care coordination?
- Are there any referrals or patient profiles that are more likely to require higher levels of care coordination, especially with external consultants/specialists?
- How well was cross-institutional provider communication supported?
- What were facilitators and barriers?
-
6
Describe any communication breakdowns with specialists both within and outside of your institution?
Impact…
-
7
How do the differences among internal and external referrals impact your choice of consultant? (In other words, is one easier than the other and does that influence your choice to make internal/external referrals).
-
8How do organizational policies affect both internal and external referrals related communication or information sharing?
- Are you familiar with communication and information sharing practices or policies at other medical centers, especially as they relate to cross-institutional physician-dyads (referrers and consultants)?
- Has that influenced the workflow here? How?
- Do you feel like you can try new things to improve your work processes?
-
9What impact, if any, do health information exchange (HIE) technologies have on your clinical work?
- How can HIE technologies change to best improve your workflow and quality of care?
-
10
In what ways do you think technology improvements reduce patient burden?
-
11
Are there any other aspects of follow-up after an internal or external process that you think we should know?
Thank you for participation!
Appendix B: Consultant Interview Guide
“This is an interview with [participant ID] on [date].”
Today, we are here to learn from you about the differences between internal and external consultation processes. During this interview, the internal consultation process describes scenarios where both the referrer and consultant are in the same healthcare institution and use the same electronic health record system (EHR). An external or cross-institutional consultation process describes scenarios where the referrer and consultant work in different healthcare institutions and do not use the same EHR.
We would like to know how your workflow differs among these two scenarios, especially for the initial consult. We would like to hear your perspective on provider communication, information technology, documentation, and workflow efficiency.
Characterize Workflow Differences
-
1
Describe your typical clinical workflow for initial consults. [Internal]
-
2How does your workflow differ when the consult was ordered from external referrers?
- Are there the same number of steps/tasks or documentation for both scenarios?
- Describe any other software applications or communication processes that are used to support the initial consult.
-
3What kind of information is needed to fully support the initial consult (i.e., clinical question, medication, referrer note, referrer contact information)?
- What are the sources of information (e.g., care team, patients, referrer)?
- How do you retrieve information needed? What modes are used to share or communicate patient information (fax, phone calls, EHR, HIE – secure emails, etc.)?
-
4How does the workflow, information flow, or communication differ when patients are referred from an external referrer?
- What are the sources of information (e.g., care team, patients, referrer)?
- How do you retrieve information needed? What modes are used to share or communicate patient information (fax, phone calls, EHR, HIE, secure emails, etc.)?
Clinical Example…
-
5Can you describe a case(s) where a patient from an external referral required a high-level of care coordination?
- Are there any referrals, consults, or patient profiles that are more likely to require higher levels of care coordination, especially with external consultants/specialists?
- How well was cross-institutional provider communication supported?
- What were facilitators and barriers?
-
6
Describe any communication breakdowns with referrers or other specialists both within and outside of your institution?
Impact…
-
7
How do the differences among internal and external referrals [to you] impact your care delivery or acceptance of referral? (Do you feel that you can deliver the same quality of care to patients from an external referral).
-
8How do organizational policies affect both internal and external consultations/referrals related communication or information sharing?
- Are you familiar with communication and information sharing practices or policies at other medical centers, especially as they relate to cross-institutional physician-dyads (referrers and consultants)?
- How has that influenced the workflow here?
- Do you feel like you can try new things to improve your work processes? If so, elaborate.
-
9What impact, if any, do health information exchange (HIE) technologies have on your clinical work? [Technologies or software that are designed to help information exchange/sharing or provider communication across healthcare institution.]
- How can HIE technologies change to best improve your workflow and quality of care?
-
10
In what ways do you think technology improvements can reduce patient burden?
-
11
Are there any other aspects of the consultation process that you think we should know?
Thank you for participation!
Footnotes
Competing interest(s): The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Declarations
Ethics approval and consent to participate: The study was approved by the Indiana University Institutional Review Board (study protocol #10493). Informed consent was obtained from all study participants and the study was carried out in accordance with relevant guidelines and regulations.
References
- 1.Ackerman SL, Gleason N, Shipman SA. Comparing patients’ experiences with electronic and traditional consultation: results from a multisite survey. Journal of general internal medicine 2020;35:1135–1142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bell SK, Folcarelli P, Fossa A, et al. Tackling ambulatory safety risks through patient engagement: what 10,000 patients and families say about safety-related knowledge, behaviors, and attitudes after reading visit notes. Journal of Patient Safety 2021;17:e791–e799. [DOI] [PubMed] [Google Scholar]
- 3.Patel MP, Schettini P, O’Leary CP, et al. Closing the referral loop: an analysis of primary care referrals to specialists in a large health system. Journal of general internal medicine 2018;33:715–721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Militello LG, Savoy A, Porter B, et al. Hidden complexities in information flow between primary and specialty care clinics. Cognition, Technology & Work 2018;20:565–574. [Google Scholar]
- 5.Institute for Healthcare Improvement. Closing the loop: A guide to safer ambulatory referrals in the EHR era. Cambridge, MA: Institute for Healthcare Improvement, 2017. [Google Scholar]
- 6.Hoffman J Malpractice risks in communication failures: 2015 annual bencmarking report. Cambridge, MA: CRICO Strategies, 2016. [Google Scholar]
- 7.Gandhi TK, Sittig DF, Franklin M, et al. Communication breakdown in the outpatient referral process. J Gen Intern Med 2000;15:626–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nehls N, Yap TS, Salant T, et al. Systems engineering analysis of diagnostic referral closed-loop processes. BMJ Open Quality 2021;10:e001603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Patel MP, Schettini P, O’Leary CP, et al. Closing the referral loop: an analysis of primary care referrals to specialists in a large health system. J Gen Intern Med 2018;33:715–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Straus SG, Chen AH, Yee H Jr, et al. Implementation of an electronic referral system for outpatient specialty care, In AMIA Annual Symposium Proceedings, American Medical Informatics Association, 2011. [PMC free article] [PubMed] [Google Scholar]
- 11.Foundation IfHINPS. Closing the Loop: A Guide to Safer Ambulatory Referrals in the EHR Era. Institute for Healthcare Improvement; 2017. [Google Scholar]
- 12.Dixon BE, Embi PJ, Haggstrom DA. Information technologies that facilitate care coordination: provider and patient perspectives. Translational Behavioral Medicine 2018;8:522–525. [DOI] [PubMed] [Google Scholar]
- 13.O’Malley AS, Reschovsky JD. Referral and consultation communication between primary care and specialist physicians: Finding common ground. Archives of Internal Medicine 2011;171:56–65. [DOI] [PubMed] [Google Scholar]
- 14.Tsai J, Yakovchenko V, Jones N, et al. “Where’s My Choice?” An Examination of Veteran and Provider Experiences With Hepatitis C Treatment Through the Veteran Affairs Choice Program. Med Care 2017;55 Suppl 7 Suppl 1:S13–s19. [DOI] [PubMed] [Google Scholar]
- 15.Savoy A, Militello L, Diiulio J, et al. Cognitive requirements for primary care providers during the referral process: Information needed from and interactions with an electronic health record system. Int J Med Inform 2019;129:88–94. [DOI] [PubMed] [Google Scholar]
- 16.Payne TH, Lovis C, Gutteridge C, et al. Status of health information exchange: a comparison of six countries. J Glob Health 2019;9:0204279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Savoy A, Patel H, Flanagan ME, et al. Comparative usability evaluation of consultation order templates in a simulated primary care environment. Applied Ergonomics 2018;73:22–32. [DOI] [PubMed] [Google Scholar]
- 18.Neal R, Tharmanathan P, France B, et al. Is increased time to diagnosis and treatment in symptomatic cancer associated with poorer outcomes? Systematic review. British journal of cancer 2015;112:S92–S107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Saleem JJ, Russ AL, Neddo A, et al. Paper persistence, workarounds, and communication breakdowns in computerized consultation management. International journal of medical informatics 2011;80:466–479. [DOI] [PubMed] [Google Scholar]
- 20.Vest JR, Gamm LD. Health information exchange: persistent challenges and new strategies. Journal of the American Medical Informatics Association 2010;17:288–294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Shen MJ, Binz-Scharf M, D’Agostino T, et al. A mixed-methods examination of communication between oncologists and primary care providers among primary care physicians in underserved communities. Cancer 2015;121:908–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kim Y, Chen AH, Keith E, et al. Not perfect, but better: primary care providers’ experiences with electronic referrals in a safety net health system. J Gen Intern Med 2009;24:614–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Fabre JC, Andresen PA, Wiltz GM. Closing the Loop on Electronic Referrals: A Quality Improvement Initiative Using the Care Coordination Model. The Journal of Ambulatory Care Management 2020;43:71–80. [DOI] [PubMed] [Google Scholar]
- 24.Savoy A, Militello LG, Patel H, et al. A cognitive systems engineering design approach to improve the usability of electronic order forms for medical consultation. J Biomed Inform 2018;85:138–148. [DOI] [PubMed] [Google Scholar]
- 25.Weiner M, Savoy A, Barker BC. Gains, losses, and uncertainties from computerizing referrals and consultations. Applied Ergonomics 2020;89:103227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Holden RJ, Voida S, Savoy A, et al. Human factors engineering and human–computer interaction: supporting user performance and experience. Clinical informatics study guide: Springer, 2016:287–307. [Google Scholar]
- 27.Carayon P, Hoonakker P. Human Factors and Usability for Health Information Technology: Old and New Challenges. Yearbook of medical informatics 2019;28:71–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Carayon P, Wetterneck TB, Rivera-Rodriguez AJ, et al. Human factors systems approach to healthcare quality and patient safety. Applied ergonomics 2014;45:14–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Carayon P, Hundt AS, Karsh B, et al. Work system design for patient safety: the SEIPS model. BMJ Quality & Safety 2006;15:i50–i58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Holden RJ, Carayon P, Gurses AP, et al. SEIPS 2.0: a human factors framework for studying and improving the work of healthcare professionals and patients. Ergonomics 2013;56:1669–1686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Halamka JD, Osterland C, Safran C. CareWeb™, a web-based medical record for an integrated health care delivery system. International journal of medical informatics 1999;54:1–8. [DOI] [PubMed] [Google Scholar]
- 32.Biondich PG, Grannis SJ. The Indiana Network for Patient Care: An Integrated Clinical Information System Informed by Over Thirty Years of Experience. Journal of Public Health Management and Practice 2004;10:S81–S86. [PubMed] [Google Scholar]
- 33.Creswell JW, Creswell JD. Research design: Qualitative, quantitative, and mixed methods approaches: Sage publications, 2017. [Google Scholar]
- 34.Landon BE, Onnela J-P, Meneades L, et al. Assessment of Racial Disparities in Primary Care Physician Specialty Referrals. JAMA Network Open 2021;4:e2029238–e2029238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Vimalananda VG, Meterko M, Waring ME, et al. Tools to improve referrals from primary care to specialty care. Am J Manag Care 2019;25:e237–e42. [PubMed] [Google Scholar]
- 36.Gale RC, Wu J, Erhardt T, et al. Comparison of rapid vs in-depth qualitative analytic methods from a process evaluation of academic detailing in the Veterans Health Administration. Implementation Science 2019;14:1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Melnick ER, Dyrbye LN, Sinsky CA, et al. The association between perceived electronic health record usability and professional burnout among US physicians, In Mayo Clinic Proceedings, Elsevier, 2020. [DOI] [PubMed] [Google Scholar]
- 38.Hingle S Electronic Health Records: An Unfulfilled Promise and a Call to Action. Annals of Internal Medicine 2016;165:818–819. [DOI] [PubMed] [Google Scholar]
- 39.Beasley JW, Wetterneck TB, Temte J, et al. Information chaos in primary care: implications for physician performance and patient safety. The Journal of the American Board of Family Medicine 2011;24:745–751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Savoy A, Patel H, Murphy DR, et al. Electronic Health Records’ Support for Primary Care Physicians’ Situation Awareness: A Metanarrative Review. Human Factors 2021:00187208211014300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Singh H, Schiff GD, Graber ML, et al. The global burden of diagnostic errors in primary care. BMJ quality & safety 2017;26:484–494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Straus SG, Chen AH, Yee H, Jr., et al. Implementation of an electronic referral system for outpatient specialty care. AMIA Annu Symp Proc 2011;2011:1337–46. [PMC free article] [PubMed] [Google Scholar]
- 43.Woodward M, De Pennington N, Grandidge C, et al. Development and evaluation of an electronic hospital referral system: a human factors approach. Ergonomics 2020;63:710–723. [DOI] [PubMed] [Google Scholar]
- 44.Savoy A, Militello LG, Patel H, et al. A cognitive systems engineering design approach to improve the usability of electronic order forms for medical consultation. Journal of biomedical informatics 2018;85:138–148. [DOI] [PubMed] [Google Scholar]