The Quest to End the Flu
The methods used to make flu vaccines are slow and sometimes unreliable, and new viruses threaten to outrun them. Can researchers find a way to stay ahead?
On April 28, 2009, a box containing a newly isolated virus showed up at Doris Bucher’s lab. She and her colleagues at New York Medical College opened it up right away. Thousands, or perhaps millions, of lives might depend on what they did next.
The virus was a new kind of influenza, known as 2009 H1N1. It had abruptly started spreading across North America in the previous month, and was beginning to appear in countries around the world. Once scientists at the Centers for Disease Control and Prevention analyzed it, they realized that the vaccine already in production for the next flu season probably wouldn’t be effective against it. And because it was so new, people’s immune systems might also be unable to stop the virus, which meant that it could become a global outbreak—a pandemic.
No one knew how bad 2009 H1N1 might prove to be, but the experts did know that the virus had the capacity to be very bad. Flu pandemics had occurred three times in the previous century, and the worst of them, the so-called Spanish Flu of 1918–19, had killed an estimated 50 million people. It, too, was an H1N1 virus. Once researchers at the CDC got hold of the 2009 H1N1 virus, they had one urgent mission: make a new vaccine.
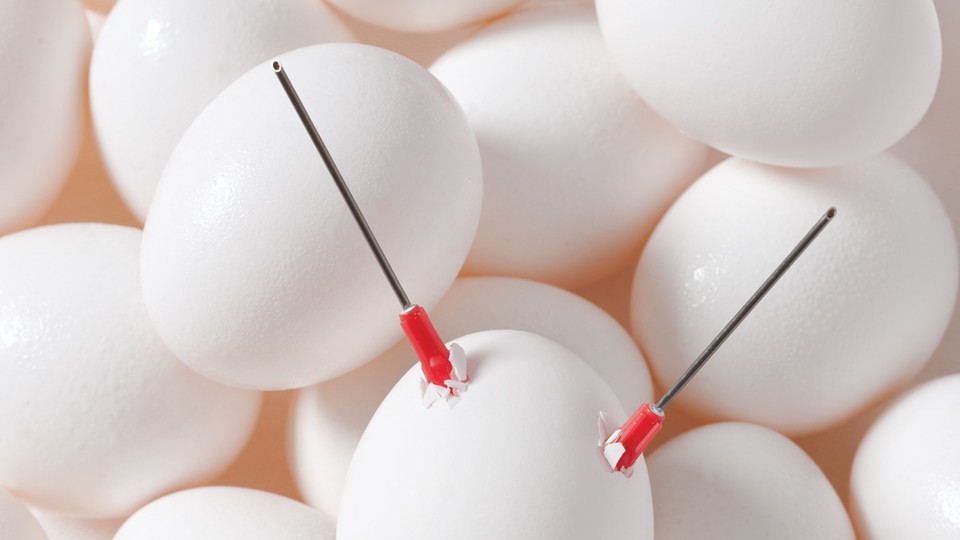
The first step was to send batches of the virus to a handful of vaccine experts like Bucher. As soon as she received her supply of 2009 H1N1, she got to work on creating a “seed stock” of modified viruses that could be used to produce hundreds of millions of vaccine doses. Manufacturers for the most part still make flu vaccines the way they did in World War II: in chicken eggs. Bucher had to transform the viruses, which grow very well in human airways, so that they would grow very well in eggs.
Bucher and her colleagues created a new seed stock using a method more than four decades old, which she has been refining in recent years, as she has helped prepare each year’s seasonal flu vaccine. She and her colleagues drilled tiny holes into the eggs and injected the 2009 H1N1 virus, along with another flu strain that grows well in eggs. The two viruses made copies of themselves in the eggs, and sometimes their genes mixed together, producing hybrids. Bucher’s team harvested the viruses from the eggs and plucked out the best-growing hybrids, reinserting the lines into new eggs. Before long, the team had produced a hybrid that could be used to inoculate people against 2009 H1N1—and could produce 32 times more virus in eggs than the strain Bucher had received in the mail. “We got this thing ready in three weeks,” Bucher told me recently, with the pride of a viral gardener. “It worked beautifully.”
But it was not until October that the first 2009 H1N1 vaccines started trickling into clinics and hospitals. Six to eight months from isolating a new flu virus to putting shots in arms is a typical schedule for a flu vaccine. Unfortunately, the virus didn’t get the memo. Cases of 2009 H1N1 were already skyrocketing in the United States—but the vaccine supply was less than half the projected amount. Many of the people clamoring for the vaccine couldn’t get it.
Bucher’s daughter was one of them. “She had a baby at the end of September, and that meant she was really at risk,” Bucher told me. “My daughter went to a vaccine site on the Upper East Side. The line went for blocks. And then she went home.” Bucher was frustrated to no end that her own daughter couldn’t get the vaccine she had created six months earlier, fewer than 30 miles away.
“I thought, This is really depressing,” says Bucher.
Fortunately, her daughter survived the pandemic, and 2009 H1N1 turned out to be a bullet dodged. In 2012, a CDC-led team of epidemiologists reviewed health records and estimated that only 284,400 people died of H1N1-related complications worldwide in the first 12 months of its wide circulation. “Only 284,400 deaths” may sound like a grotesque downplaying of a huge loss of life, until you consider that the 1918 pandemic killed, according to some estimates, nearly 200 times as many people.
The relatively low death toll was not the result of a hugely effective vaccine that stopped a deadly virus. In a 2013 study, CDC researchers estimated that the vaccine was only 62 percent effective in people younger than 65. (For those older than 65, it was only 43 percent effective.) While that’s far better than zero, it’s mediocre compared with the effectiveness of vaccines for diseases like polio and measles, which can reduce a person’s risk of infection by more than 90 percent.
To make matters worse, only an estimated
27 percent of people in the United States ended up getting the vaccine for 2009 H1N1 by April 2010, in part because it didn’t start arriving in sufficient numbers until the end of December. (During last year’s flu season, 45 percent of people older than six months got vaccinated.) So the vaccine was just a modest help for public health: Between
43 million and 89 million people in the United States came down with 2009 H1N1 from April 2009 to April 2010. The vaccine prevented 700,000 to 1.5 million cases. Between 8,870 and 18,310 people in the United States are estimated to have died in the pandemic. The vaccine thus saved 200 to 500 lives.
It turned out that 2009 H1N1 had little trouble spreading, but a lot of trouble killing on a massive scale. A future flu virus might have much less trouble. We have been warned.
The frustrations of 2009 showed experts just how mysterious flu viruses can be, and how much vaccines against them leave to be desired. The sudden outbreak drove home the realization that the world needs vaccines that are more effective and faster to make—not just to reduce the 250,000 to 500,000 deaths from seasonal flu that occur every year but also to prepare for the arrival of new, deadly pandemics. Many researchers became convinced that it was time to step beyond World War II–era technology and start using 21st‑century methods for making vaccines. “The eggs should be long gone,” grumbles Michael Osterholm, the director of the Center for Infectious Disease Research and Policy at the University of Minnesota.
In the four years since the 2009 pandemic, researchers have been searching furiously for a better answer. This year saw the publication of a string of papers that could lead scientists to a fundamentally new kind of flu vaccine—one that might someday substantially reduce the impact of a pandemic, and save many lives that would otherwise be lost to seasonal flu.
Most scientists call it a universal flu vaccine, because it would protect people against many flu strains, including ones that have yet to evolve. This universal vaccine could ultimately put an end to the annual ritual of getting a flu shot: each jab might protect for years or even a lifetime.
It could take years, even a lifetime, before a universal flu vaccine becomes available. Still, the mere fact that it could become a reality marks an important shift in the fight against influenza. “We don’t have them ready to go tomorrow,” says Anthony Fauci, the director of the National Institute of Allergy and Infectious Diseases, of the next generation of vaccines. “But we didn’t even have them at the concept stage in 2009.”
In its own day, the chicken-egg flu vaccine was a headline-grabbing triumph. Medical researchers first started looking for a flu vaccine during the carnage of the 1918 pandemic. But all attempts to create one failed, and for a very simple reason: no one knew what caused influenza. It wasn’t until 1933 that British researchers first isolated a strain of the virus.
Scientists had discovered that they could create an abundant supply of viruses to study by injecting them into chicken eggs, and flu researchers started doing the same. As scientists came to understand the biology of the flu virus better, they started testing egg-grown viruses as vaccines. Injected into people’s arms, the vaccine viruses, doused with chemicals to inactivate them, triggered a protective immune response. The U.S. military took over flu-vaccine research during World War II, fearing that a 1918-scale pandemic would paralyze the Army. In 1943, American soldiers rolled up their sleeves and started getting an early flu shot.
The flu vaccine raised hopes that deadly pandemics would become a thing of the past. But it proved to be remarkably fickle. Vaccines for other diseases typically protected people for decades—even for life. The flu vaccine’s protection could abruptly fade away.
The reason for this failure, it would turn out, is that flu viruses are especially good at evading vaccines. When we get a flu vaccine, our immune system responds by making antibodies. Later, if we get infected by a flu virus, the antibodies attack it. Most of the antibodies will latch on to the tips of proteins that stud the surface of the virus, interfering with the virus as it tries to invade our cells.
But a flu virus mutates at an exceptionally high rate as it reproduces, and some mutations will change the tips of the surface proteins. The antibodies cannot grab tightly to the altered tips, so the virus is able to proceed with its invasion. From one flu season to the next, the evolution of the flu renders last season’s vaccine useless. The only way to protect people against a new year’s flu is to give them a new vaccine. On a chart of vaccine schedules, the flu vaccine’s stands out as the only one that requires annual injections. “There’s really nothing else like it,” says Richard Webby, a virologist at St. Jude Children’s Research Hospital in Memphis, Tennessee.
The World Health Organization monitors flu strains as they rise to dominance, and each February it convenes a meeting to recommend which strains should go into the vaccine for the next flu season in the Northern Hemisphere. In September, it meets again to make the same decision for the Southern Hemisphere.
There are many ways for a year’s vaccine production to go wrong. The vaccine may turn out to work worse than expected. When scientists adapt viruses to grow better in eggs, the viruses mutate in ways that are not possible in viruses outside the lab. The viruses that go into a vaccine can thus provoke antibodies that are mismatched with the viruses it’s supposed to fight. In some years, the eggs themselves become infected with pathogens, wiping out millions of doses.
Even in good years, the flu vaccine does worse than vaccines for other diseases like measles or polio. Last year, Osterholm and his colleagues at the University of Minnesota surveyed a number of studies on standard flu-vaccine shots. For adults younger than 65, they estimated that flu shots are 59 percent effective. As people get older, their immune system grows weaker, and so effectiveness wanes in people older than 65. Most people who die of the seasonal flu are older than 65; some studies suggest that a vaccine lowers the number of flu-related deaths in this group by as little as 5 percent.
Rather than make a risky investment to research a vastly more effective flu vaccine, producers have continued to fine-tune the existing one. “There’s no incentive to make something better, more reliable,” Anthony Fauci says. “It doesn’t make companies rich.”
Osterholm and his colleagues recently asked vaccine-producing companies what it would cost to make a better flu vaccine. The answers they got led them to make an estimate of up to $1 billion. “We found no one who had an appetite for that,” Osterholm says.
New pandemics don’t come out of the blue. They evolve from viruses that infect animals—typically birds. Every now and then a bird-flu virus infects a person—a chicken dealer in a Shanghai marketplace, for example. The virus may or may not make that person sick, but one thing is almost certain: it won’t be able to get from that person to another person. Almost certain. Bird-flu viruses live in the guts of birds, and so they adapt poorly to living in the human airway. But on very rare occasions, a bird flu makes the leap over the species barrier and turns into a human flu, and then spreads easily from person to person. Once a bird flu evolves into a human flu, it can start spreading around the world in a new pandemic. It may kill thousands or millions.
Faced with sudden bird-flu outbreaks in the mid‑2000s, the U.S. government began launching new programs to find better ways of making flu vaccines. Those programs were just getting off the ground when the 2009 H1N1 pandemic struck—but they were not mature enough to help fight the flu that year. Now they are starting to yield tangible changes.
Among the flu vaccines available in the United States this year is one called Flucelvax, made by Novartis. Flucelvax is not produced in chicken eggs. Novartis makes it in massive stainless-steel tanks that contain warm broths of flu-infected cells grown from a dog kidney (cells, Novartis emphasizes, that were taken from a single kidney decades ago and then reproduced).
Making vaccines in mammalian cells has many potential advantages over making them in eggs. The viruses may be less likely to come out mismatched to the strains making people sick. The factories don’t have to worry about eggs becoming infected with pathogens that can ruin a whole batch of vaccine. Flu experts also expect that mammalian cells will make it easier to scale up vaccine production in the face of a deadly pandemic. To make hundreds of millions of vaccine doses with eggs, manufacturers have to get hold of hundreds of millions of chicken eggs from chicken farmers; a cell-based factory just needs to build new tanks and inoculate them with fast-growing mammalian cells.
Phil Dormitzer, the head of Novartis Vaccines’ virology and U.S.-vaccine-research programs, sees the new factories as bringing flu vaccines into the modern pharmaceutical age. But with just two cell-based factories (one in North Carolina and the other in Germany), the company is still making most of its flu vaccines in chicken eggs this year. “We’re going to have to prove that the technology is reliable year after year before anyone is going to be willing to shut down egg-based plants,” Dormitzer told me.
While Fauci, of the National Institute of Allergy and Infectious Diseases, says that Novartis’s cell-based factories are a big step in the right direction, he doesn’t consider them a clean break with traditional ways of making flu vaccines. Fauci is more excited about something called a recombinant protein vaccine, which does not rely on growing viruses, even though it is cell-based. At Protein Sciences, a small Connecticut biotech firm, researchers isolate the gene for the flu virus’s surface proteins and insert it into an entirely different species of virus, called a baculovirus. The baculovirus infects insect cells and causes them to make huge amounts of the surface proteins, which the company uses to make Flublok, the only recombinant protein flu vaccine currently available.
Yet all cell-based flu vaccines share the same shortcoming: they’re not very effective. A 2011 study at the University of Rochester found that Flublok, for example, was 44.6 percent effective. And the protection from these new flu vaccines fades away in a year, just like vaccines from chicken eggs. That’s because cell-based vaccines cause people to make antibodies to the tips of the surface proteins—the same kind of antibodies that flu vaccines have been producing for 70 years. “It’s like putting a 1940s transmission in a 2014 car,” Osterholm says.
What these faster vaccine factories need is a better vaccine to make. “The ideal would be to have one flu vaccine that you use once to become immunized for life and be protected against every new kind of flu,” says Barney Graham of the Vaccine Research Center at the National Institute of Allergy and Infectious Diseases.
Recent research suggests that the longtime dream of a universal flu vaccine could eventually come true. Instead of targeting the tips of the surface proteins, this kind of vaccine would target a part of the virus that doesn’t change so easily. Scientists have discovered that the stems of the surface proteins change very little. A stem vaccine might provide protection against many different kinds of flu—protection that could last for years or decades. To test this idea, scientists have engineered antibodies that latch tightly to the stems. So far, mice injected with these stem antibodies can resist infection—not just by one strain but by many. If scientists can create a vaccine that provokes us to make these stem antibodies, they could provide broad protection against the flu.
At the Icahn School of Medicine at Mount Sinai, in New York City, Peter Palese is leading experiments to get mice and ferrets to make their own stem antibodies. The researchers have tried various methods, including the same one used to make Flublok—insect cells churning out surface proteins. But the cells engineer the proteins in a special way, creating several different forms. Each form has a tip from a different strain of flu, while they all have the same stem. When Palese and his colleagues inject this cocktail into an animal, its immune system is exposed to many protein tips, but the same stem. So the immune system responds with an abundance of stem antibodies. Palese and his colleagues have injected a wide range of flu strains into vaccinated animals. In every case, the animals can fight off a lethal dose.
Fauci and other researchers hope to push this research toward clinical trials in humans. If a universal vaccine proves to be safe and effective, doctors might eventually be able to dispense it every few years, or just a couple of times to children for lifetime protection. The vaccine might protect against new flu pandemics, doing away with the dangerous lag time currently required for making new vaccines. “We could actually get ahead of pandemics,” Osterholm says.
But the history of flu vaccines leaves many experts unwilling to hold their breath. “It’s not a matter of finding a result in a lab today and having a product tomorrow,” St. Jude’s Richard Webby warns. “These things can take decades to get through.”
Palese acknowledges that the vaccine may fail in clinical trials. “Mice are not men, and the immune systems are different,” he says. “Unless we can get it into humans, the jury is still out.”
While Palese and his colleagues were running their experiments, two men in Shanghai died of the flu last March. It turned out that they were both infected with H7N9, a subtype of bird flu never seen before in humans. Since then, H7N9 has turned up throughout eastern China and in Taiwan. Out of the 136 people who had fallen ill as of mid-October, 45 died.
H7N9 infects chickens without making them sick, and so it has been able to spread invisibly. So far, only one case of probable human-to-human transmission has been found. But H7N9 might not need more than a few mutations to move easily from one person to another.
As H7N9’s worrying nature became clear, the U.S. Department of Health and Human Services started a program to develop a vaccine, commissioning the vaccine manufacturer Sanofi Pasteur to grow H7N9 viruses. Last September, the National Institute for Allergy and Infectious Diseases launched a clinical trial with a vaccine made from those viruses. If the vaccine proves effective, the government may create a stockpile to use in case the virus turns into a pandemic.
The stockpile would be for first responders only, though, and it wouldn’t be ready this winter. Nor will any of the advanced flu-vaccine factories now using dog cells or insect cells produce an emergency supply of vaccines for a pandemic: they don’t have the capacity. And so the H7N9 vaccine is being made the old-fashioned way. At Sanofi Pasteur, people are carefully drilling holes into chicken eggs.
The trials of the H7N9 vaccine should be done by late 2014. If the government goes ahead with manufacturing a stockpile, it will need millions more eggs, and months more time. But if history has taught us anything, it’s that influenza does not respect our timetables.