


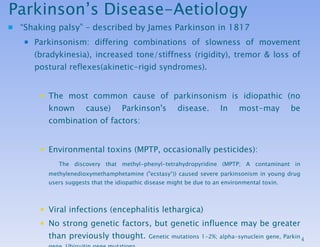











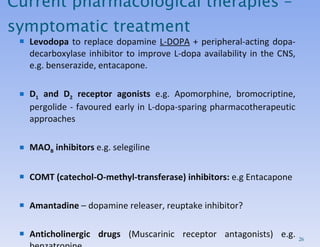
![Investigations: The diagnosis is made clinically, as there is no diagnostic test for Parkinson's disease. Imaging (CT or MRI) of the head may be needed if there are any features suggestive of pyramidal, cerebellar or autonomic involvement, or the diagnosis is otherwise in doubt (e.g to exclude stroke). [ 18 F]dopa PET and β-CIT SPECT images. [ 18 F]dopa PET uptake in the putamen is reduced in PD.](https://image.slidesharecdn.com/parkinson-100715002508-phpapp02/85/Parkinsons-Disease-18-320.jpg)



















Parkinsons Disease
- 2. Lecture Outline Aetiology Incidence Patho-physiology Clinical Presentation Diagnosis Prognosis Treatment Exam prep-what to know!
- 4. Parkinson’s Disease-Aetiology “ Shaking palsy” – described by James Parkinson in 1817 Parkinsonism: differing combinations of slowness of movement (bradykinesia), increased tone/stiffness (rigidity), tremor & loss of postural reflexes(akinetic-rigid syndromes). The most common cause of parkinsonism is idiopathic (no known cause) Parkinson's disease. In most-may be combination of factors: Environmental toxins (MPTP, occasionally pesticides): The discovery that methyl-phenyl-tetrahydropyridine (MPTP; A contaminant in methylenedioxymethamphetamine ("ecstasy“)) caused severe parkinsonism in young drug users suggests that the idiopathic disease might be due to an environmental toxin. Viral infections (encephalitis lethargica) No strong genetic factors, but genetic influence may be greater than previously thought. Genetic mutations 1-2%; alpha-synuclein gene, Parkin gene, Ubiquitin gene mutations. Protective factors-Both smoking and coffee drinking have been associated with a lower risk for PD.
- 5. PARKINSON'S DISEASE-Incidence Annual incidence 0.2/1000 & prevalence of 1.5/1000. Prevalence rates are similar throughout the world, except lower rates in China /West Africa. Affects 1% of those over 55 years, 1.5% of people 70-79 years of age Generally occurs between 50-80 years Sex incidence is about equal.
- 7. Pathology There is depletion of the pigmented dopaminergic neurons in the substantia nigra, atrophic changes in the substantia nigra& depletion of neurons in the locus coeruleus. Clinical features don’t emerge until >60-80% dopamine lost. Compensatory changes include hyperactivity in remaining neurones (increased transmitter turnover), increase in dopamine receptors; receptor supersensitivity Other pigmented nuclei also affected (locus ceruleus and raphe). Also cortex and other structures affected. Characteristic histological inclusion in affected neurons are eosinophilic cytoplasmic inclusions in nigral cells called the Lewy Bodies.
- 8. Parkinson’s Disease-Patho-physiology Basal Ganglia Controls movement Dopamine Inhibitory neurotransmitter in the basal ganglia Acetylcholine Excitatory neurotransmitter in the basal ganglia Without dopamine, inhibitory influences are lost and excitatory mechanisms are unopposed Neurons of basal ganglia are over stimulated Excess muscle tone, tremors & rigidity Extrapyramidal system next lecture!
- 10. Parkinson’s Disease- Clinical features: The classical syndrome: Tremors Rigidity Bradykinesia These may be absent initially, when non-specific symptoms of tiredness, aching limbs, mental slowness, depression & small handwriting (micrographia) may be noticed. Although parkinsonian features are initially unilateral, gradual bilateral involvement is the rule. A resting tremor in an upper limb being a common presenting feature.
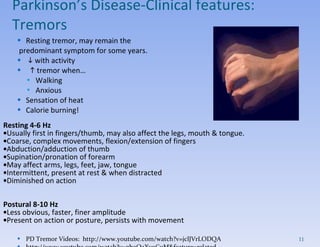
- 11. Resting tremor, may remain the predominant symptom for some years. with activity tremor when… Walking Anxious Sensation of heat Calorie burning! Resting 4-6 Hz Usually first in fingers/thumb, may also affect the legs, mouth & tongue. Coarse, complex movements, flexion/extension of fingers Abduction/adduction of thumb Supination/pronation of forearm May affect arms, legs, feet, jaw, tongue Intermittent, present at rest & when distracted Diminished on action Postural 8-10 Hz Less obvious, faster, finer amplitude Present on action or posture, persists with movement PD Tremor Videos: http://www.youtube.com/watch?v=jclJVrLODQA http://www.youtube.com/watch?v=gboQaXv9CuM&feature=related Parkinson’s Disease- Clinical features: Tremors
- 12. Parkinson’s Disease- Clinical features: Rigidity Cogwheel type, mostly upper limbs - Rigidity with superimposed tremor, felt as tigthness/stiffness of muscles, Ratchet-like (catch-release-catch release like movement. Plastic (leadpipe) type, mostly legs Stiffness Neck Trunk Shoulders Posture Head bowed Body bent forward Arms flexed Thumbs turned into palms Knees bent (slightly)
- 13. Paul Marie Louis Pierre Richer (1849-1933) was a French anatomist, physiologist, sculptor and anatomical artist. Paul Richer was an assistant to Jean-Martin Charcot at the Salpêtrière. In 1880, Jean-Marie Charcot completed a full clinical description of Parkinson's Disease. The symptoms were depicted by Paul Richer in drawings and a statuette of people with Parkinson's Disease. Along with a photograph, these are the first known depictions of Parkinson's Disease Parkinson’s Disease- Clinical features: Rigidity
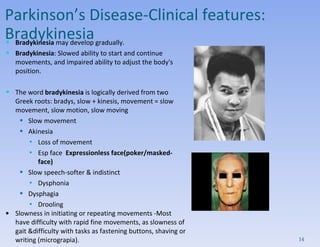
- 14. Bradykinesia may develop gradually. Bradykinesia : Slowed ability to start and continue movements, and impaired ability to adjust the body's position. The word bradykinesia is logically derived from two Greek roots: bradys, slow + kinesis, movement = slow movement, slow motion, slow moving Slow movement Akinesia Loss of movement Esp face Expressionless face(poker/masked-face) Slow speech-softer & indistinct Dysphonia Dysphagia Drooling Slowness in initiating or repeating movements -Most have difficulty with rapid fine movements, as slowness of gait &difficulty with tasks as fastening buttons, shaving or writing (micrograpia). Parkinson’s Disease- Clinical features: Bradykinesia
- 15. Asymmetrical Gait Slow to start walking Shortened stride Stiff legged gait-rigidity comes through on one side, therefore difficult clearing swinging on one side Rapid, small steps, tendency to run (festination) Reduced arm swing (usually unilateral) Impaired balance on turning Leads with head and shoulders Fall forward down turned posture- Postural righting reflexes are impaired early, but falls tend not to occur until later. Parkinson’s Disease- Clinical features: Abnormal Gait/posture PD Gait Videos: http://www.youtube.com/watch?v=_6u2W1mzCeM http://www.youtube.com/watch?v=ylHZWO17W70&NR=1
- 16. Additional information to read later Clinical features: There are a number of abnormalities on neurological examination: Muscle strength / reflexes remain normal, plantar responses are flexor. There is a paucity of facial expression (hypomimia) & the blink reflex may be exaggerated & fail to habituate (glabellar tap sign). Eye movements are normal to standard clinical testing, provided allowance is made for the normal limitation of upward gaze with age. Sensation is normal & intellectual abilities are not affected initially. As the disease progresses, 1/3 develop cognitive impairment. PD commonly associated with other features; loss of smell, depression, dementia, autonomic dysfunction, sleep disturbance- due to involvement of other non-dopaminergic structures as disease progresses.
- 18. Investigations: The diagnosis is made clinically, as there is no diagnostic test for Parkinson's disease. Imaging (CT or MRI) of the head may be needed if there are any features suggestive of pyramidal, cerebellar or autonomic involvement, or the diagnosis is otherwise in doubt (e.g to exclude stroke). [ 18 F]dopa PET and β-CIT SPECT images. [ 18 F]dopa PET uptake in the putamen is reduced in PD.
- 19. Investigations: Causes of parkinsonism: Toxins (manganese, CO poisoning), CNS infs, structural lesions, metabolic disorders, other neurologic disorders. Most are rare& suggested by atypical features, history or exam. Routinely needed to consider 2 alternative diagnoses: Drug-induced parkinsonism “ Parkinsonism-plus” syndromes: parkinsonian features with other neurological signs atypical of parkinson disease.
- 20. Drug-induced parkinsonism: Important because it is reversible, although may require weeks or months after discontinuation. Dopamine antagonists;neuroleptic agents (HALPERIDOL), atypical neuroleptic agents, antiemetic drugs, CCB (flunarizine ,cinnarizine). Amiodarone, valproic acid,lithium,by uncertain mechanisms. Dopamine antagonists also exacerbate Parkinson’s disease& should be avoided, if possible, in the treatment of patients with the disease.
- 21. Additional information to read later Parkinson-plus syndromes:
- 22. Features suggesting other conditions include: Falls or dementia early in the course of the disease Symmetric parkinsonism Wide-based gait Abnormal eye movements Babinski signs Marked orthostatic hypotension Urinary retention Development of marked disability within 5 ys after the onset. Responds poorly to antiparkinsonians, have a worse prognosis than idiopathic PD. Neurologic consult needed if the clinical features suggest other diagnosis. Additional information to read later Parkinson-plus syndromes:
- 24. Prognosis: Variable& depends partly on the age of onset. If symptoms start in middle life, the disease is usually slowly progressive & likely to shorten lifespan because of the complications of immobility & tendency to fall. Onset after 70 is unlikely to shorten life or become severe.
- 26. Current pharmacological therapies – symptomatic treatment Levodopa to replace dopamine L-DOPA + peripheral-acting dopa-decarboxylase inhibitor to improve L-dopa availability in the CNS, e.g. benserazide, entacapone. D 1 and D 2 receptor agonists e.g. Apomorphine, bromocriptine, pergolide - favoured early in L-dopa-sparing pharmacotherapeutic approaches MAO B inhibitors e.g. selegiline COMT (catechol-O-methyl-transferase) inhibitors: e.g Entacapone Amantadine – dopamine releaser, reuptake inhibitor? Anticholinergic drugs (Muscarinic receptor antagonists) e.g. benzatropine
- 27. L-DOPA (LEVODOPA) L-3,4-hydroxyphenylalaninine (L-DOPA) a precursor of dopamine. Although the number of dopamine-releasing terminals in the striatum is diminished in Parkinson's disease, remaining neurons can be driven to produce more dopamine by administering its precursor, L-DOPA. D-DOPA is not active as a pro-drug. Well absorbed from gut, but > 90% is decarboxylated to dopamine peripherally in GIT& blood vessels & only a small proportion reaches the brain (dopamine does not readily cross BBB). Therefore combined with peripheral decarboxylase inhibitor that does not cross the blood-brain barrier along with L-DOPA . 2 peripheral decarboxylase inhibitors, carbidopa & benserazide, are available as combination preparations with levodopa, as Sinemet & Madopar, respectively. L-DOPA
- 28. The initiation of levodopa should be delayed until there is significant disability, since there is concern regarding long-term side-effects. Some suggest to initiate treatment with a dopamine agonist or a slow-release levodopa to minimise or delay the onset of long-term side-effects. 90% of patients show improvement of rigidity and bradykinesia and (to a lesser extent) tremor. 20% restored to normal motor function The initial dose is 50 mg 8-hourly, increased if necessary. The total levodopa dose may be increased to over 1000 mg/day, but should be kept as low as possible. Effective on a 3x/day regime with smooth control even though phamacological T1/2 = 90min i.e biological T1/2 >> pharmacological T1/2 initially. L-DOPA (LEVODOPA): dose/therapeutic effects
- 29. L-DOPA (LEVODOPA): unwanted effects Acute effects (tend to disappear over first few weeks): The peripheral conversion of levodopa is responsible for the high incidence of side-effects if used alone. Nausea and anorexia, hypotension, psychological effects (confusion, insomnia, euphoria, inappropriate behaviours, nightmares, hallucinosis, psychosis) Reduced by the use of a peripheral dopamine antagonist as domperidone.
- 30. Slowly developing unwanted effects, motor fluctuations. Late deterioration despite levodopa occurs after 3-5 years in 1/3-1/2. manifests as fluctuation in response; of 2 types: End-of-dose deterioration due to progression of the disease& loss of capacity to store dopamine, often can be improved by dividing the levodopa into smaller but more frequent doses, or by converting to a slow-release preparation ‘ On-off' phenomenon: More complex fluctuations present as sudden, unpredictable changes in response, in which periods of severe parkinsonism alternate with dyskinesia&agitation,is difficult to treat, but sometimes SC apomorphine (a dopamine agonist) are helpful to 'rescue' the patient rapidly. L-DOPA (LEVODOPA): unwanted effects
- 31. L-DOPA (LEVODOPA): unwanted effects Slowly developing unwanted effects, motor fluctuations. Develop in most patients after 3-5years on L-dopa, esp if young, high dose Involuntary movements, sp orofacial dyskinesias, limb &axial dystonias,occasionally depression, hallucinations& delusions. Involuntary movements (dyskinesia), can be violent; may occur as a peak-dose phenomenon, or as a biphasic phenomenon (during build-up & wearing-off phases). Management is difficult, but again involves modifying the way levodopa is administered (reduce dose) to obtain constant levels in the brain & use of alternatives, particularly dopamine agonists. Thought to be related to the short phamacological T1/2 of L-dopa causing pulsatile stimulation of the striatum and eventual disordered basal ganglia output. Dopamine dysregulation syndrome (DDS) dysfunction of the reward system, characterized by self-control problems such as addiction to medication, gambling, or hypersexuality.
- 32. Optimization of PD pharmacological treatment Now aim to prolong the pharmacological dopaminergic stimulation of the striatum to limit the development of motor fluctuations In younger patients, preference is given to neuroprotective and L-DOPA sparing therapies. L-DOPA should only be started to help overcome significant disability. In young (<65) aim to avoid L-DOPA for as long as possible (although all patients eventually need it) and tend to use long-acting (t1/2 8+hrs) dopamine agonists initially. L-DOPA plus… Peripheral COMT inhibitors, e.g. entacapone MAO B inhibitors, e.g. selegiline; may retard progression of disease D 1 and D 2 receptor agonists
- 33. Anticholinergic therapy Redressing the balance between dopaminergic and cholinergic neurons appears to be some compensation for the overall deficit in dopamine function Highest content of brain ACh is in the striatum ACh release is strongly inhibited by dopamine (D 2 receptors) Cholinergic hyperactivity due to lack of dopamine contributes to hypokinesia, rigidity and tremor (mainly via over-stimulation of the indirect pathway)
- 34. Muscarinic receptor antagonists (anticholinergic’s) These have a useful effect on tremor & rigidity, but do not help bradykinesia. They can be prescribed early in the disease before bradykinesia is a problem, but should be avoided in elderly patients in whom they cause confusion/dementia/hallucinations. Other side-effects include dry mouth, blurred vision, difficulty with micturition / constipation. Many anticholinergics are available-, trihexyphenidyl (benzhexol; 1-4 mg 8-hourly) , orphenadrine (50-100 mg 8-hourly). Trihexyphenidyl Orphenadrine Anticholinergics therapy
- 35. Amantadine While the mechanism of action of amantadine in the treatment of PD is not known, it is believed to release brain dopamine from nerve endings making it more available to activate dopaminergic receptors. This has a mild, usually short-lived effect on bradykinesia, but may be used early in the disease before more potent treatment is needed. The dose is 100 mg 8- or 12-hourly. Side-effects include nausea, dizziness (lightheadedness) and insomnia, livedo reticularis (a mottled reticulated vascular pattern that appears like a lace-like purplish discoloration of the lower extremities), peripheral oedema, confusion, seizures. Adantadine
- 36. MAO B inhibitors: Selegiline Selegiline and rasagiline belong to a class of drugs called monoamine oxidase inhibitors (MAOIs). They slow the breakdown of dopamine in the brain. They have a fairly mild anti-Parkinsonian effect in their own right . There has been some doubt as to its safety, but this is also controversial and the subject of ongoing research. The usual dose is 5-10 mg in the morning. Selegiline has an amphetamine-like metabolite (by-product). This means it can cause insomnia and hallucinations in some people. In the periphery MAO A breaks down dietary tyramine (found in cheeses, smoked meats, fish, red wine, etc.) – if you also block MAOA, will get tachycardia, hypertension, vomiting, headache) Selegiline
- 37. COMT (catechol-O-methyl-transferase) inhibitors : Entacapone prevents COMT from metabolizing L-DOPA into 3-methoxy-4-hydroxy-L-phenylalanine (3-OMD) in the periphery, which does not easily cross the blood brain barrier (BBB). Pharmacologically, entacapone is somewhat similar to carbidopa or benserazide . Entacapone (200 mg with each dose of levodoa) prolongs the effects of each dose & reduces motor fluctuations when used with levodopa. This allows the levodopa dose to be reduced & given less frequently. Entacapone
- 38. Dopamine receptor agonists : More easily administered drugs include bromocriptine (D2 receptor agonist, mild D1 receptor antagonist); pergolide (D1/D2 receptor agonist, more potent and longer acting) These drugs are less powerful than levodopa in controlling features of parkinsonism, but they are much less likely to cause dose fluctuations or dyskinesia, though they will certainly exacerbate the latter once these have developed. Side-effects include nausea, vomiting, confusion and hallucinations. Orally administered; The dose of bromocriptine is 1 mg initially, increased to 2.5 mg 8-hourly, up to 30 mg/day. Pergolide dose starts at 50 μg, increased to 250 μg 8-hourly, possibly to 3000 μg/day. Dopamine agonists derived from ergot (e.g. pergolide / cabergoline) have recently been associated with the development of cardiac fibrosis -fibrotic reactions/ thickening of heart valves, so most are screened with echo, chest X-ray / renal function tests before commencing therapy&every 6 months Bromocriptine Pergolide
- 39. Dopamine receptor agonists : Apomorphine Apomorphine given alone causes marked vomiting & has to be administered parenterally. The vomiting can be overcome by the concomitant use of the anti-sickness drug domperidone, & parenteral administration achieved through continuous subcutaneous infusion from a portable pump, or direct injection as needed. This requires considerable nursing support but, if used correctly, can be very useful. Apomorphine
- 40. Additional information to read later: Alternative treatment approaches Surgery : Stereotactic thalamotomy can be used to treat tremor, though this is needed relatively infrequently because of the medical treatments available. Other stereotactic lesions are currently undergoing evaluation, in particular pallidotomy to help in the management of drug-induced dyskinesia. Implantation of dopamine rich fragments of brain into the striatum Implantation of stem cells Midbrain neurones transplanted into the striatum Immortalised neuronal precursor cells Physiotherapy& rehab: Patients at all stages of Parkinson's disease benefit from physiotherapy, which helps reduce rigidity& corrects abnormal posture. Speech therapy may help in cases where dysarthria & dysphonia interfere with communication. Gene therapy Transfection of tyrosine hydroxylase gene into the brain
- 41. Exam prep-what to know! Describe the clinical symptoms associated with Parkinson’s disease Explain the neurotransmitter balance theory in Parkinson’s disease List the drug treatments used to treat Parkinson’s disease, indicating their mechanism of action, rationale for use and side effects.
- 42. That’s all folks (from me) Extra-Reading web resources: http://www.parkinsonindia.org/ http://www.dana.org/news/brainhealth/detail.aspx?id=9860 http://viartis.net/parkinsons.disease/treatments.htm http://www.lifespan.org/adam/indepthreports/10/000051.html
Editor's Notes
- #5: VCP3042; 1st August 2008 [email_address] Slightly more Caucasians and males Like Alzheimer’s disease, the incidence of PD is lower in smokers Death – medical complications 12-15 years or 1-3 years… variable Mutations in Alpha synuclein and Parkin genes May be induced by drugs or toxins (e.g. MPTP), and major tranquillizers cause extrapyramidal side effects, e.g. neuroleptics; manganese and CO produce extrapyramidal effects Exposure to pesticides increased risk for developing PD by 70% (Ascherio et al., 2006). Neuromelanin; oxidation of DA Increased Fe2+ in SN, decreased transferrin = increased oxidation Increased lipid peroxidation
- #27: VCP3042; 1st August 2008 [email_address] Start low and go slow! Education, physical and speech therapy, dietary modifications In Australia, l-dopa is not available without peripheral DDC inhibitors Anti-cholinergics will worsen dementia M receptor antagonists, e.g. benzatropine; modest effect, only used at the beginning to delay l-dopa; better for tremor D-dopa not converted to dopamine in vivo, and causes granulocytopaenia
- #28: VCP3042; 1st August 2008 [email_address] L-dopa effectiveness gradually declines as time progresses (2-5 years) (may rely on presence of functional dopaminergic neurones) Converted and metabolised in gut and in plasma by DDC, MAO, COMT Carbidopa and benserazide inhibit aromatic L-amino acid decarboxylase , which converts L-DOPA into , which cannot cross the BBB. Awakenings. It tells the true story of British neurologist Oliver Sacks, fictionalized as American Malcolm Sayer and portrayed by Robin Williams who, in 1969, discovers beneficial effects of the then-new drug L-Dopa. He administered it to catatonic patients who survived the 1917-1928 epidemic of encephalitis lethargica. Encephalitis lethargica or von Economo disease is an atypical form of encephalitis. Also known as &quot;sleepy sickness&quot; or as &quot;sleeping sickness&quot; (though different from the sleeping sickness transmitted by the tsetse fly), it was first described by the neurologist Constantin von Economo in 1917.[1][2] The disease attacks the brain, leaving some victims in a statue-like condition, speechless and motionless.[3] Between 1915 and 1926,[4] an epidemic of encephalitis lethargica spread around the world; no recurrence of the epidemic has since been reported, though isolated cases continue to occur.[5][6]
- #30: VCP3042; 1st August 2008 [email_address] Diminished window between wanted effect – reduced rigidity – and unwanted effect – dyskinesia (involuntary writhing) On-off effect – fluctuat es from being symptom free to having full blown symptoms Implementation of drug holidays is controversial
- #33: VCP3042; 1st August 2008 [email_address] Peripheral dopa decarboxylase inhibitors p enetrate only weakly into CNS, therefore stop conversion in periphery only; reduce dose by ¼ or a 1/5 th , reduce dopamine-induced emesis Inhibitors of dopamine degradation in the CNS by MAO, s elective for MAO B (CNS – lacks peripheral side effects); may retard progression of disease (protecting against free-radical induced neurotoxicity and apoptosis) Inhibitors of dopamine degradation in the periphery by COMT, e.g. entacepone (peripheral only); tolcapone is able to penetrate the CNS When you have a peripheral decarboxylase inhibitor this shifts the metabolism of L-dopa to the COMT pathway; COMT converts L-dopa to 3-O-methyldopa, compete with L-dopa to cross the BBB (may also contribute to the development of motor dysfunctions) Increase the amount of L-dopa available to cross the blood brain barrier Antagonists of peripheral dopamine receptors (reduce side effects)
- #34: VCP3042; 1st August 2008 [email_address] Redressing the balance between dopaminergic and cholinergic neurons appears to be some compensation for the overall deficit in dopamine function
- #36: Amantadine – less effective; better for bradykinesia and rigidity; some patients develop tachyphylaxis – drug holiday
- #39: Bromocriptine: D2 receptor agonist, mild D1 receptor antagonist Pergolide: D1/D2 receptor agonist, more potent and longer acting