ABSTRACT
Background: Common bile duct (CBD) stones are known to complicate 10-15% of gallstone diseases. Endoscopic retrograde cholangiopancreatography (ERCP) is the therapeutic modality of choice for bile duct clearance in CBD stones but may fail to achieve stone clearance. This prospective study was done to identify the predictors of failure of CBD clearance with ERCP.
Objective: This prospective study was done to identify the predictors of failure of CBD clearance with ERCP.
Methods: All consecutive patients with bile duct stones undergoing ERCP at a tertiary care center were prospectively included from October 2020 to October 2021. The study’s primary outcome was to identify and analyze factors that could predict the failure of complete CBD clearance.
Results: A total of 120 patients (50.8% males, median age: 53.5 years) were included in the final analysis. Successful clearance of CBD stones during the index procedure was achieved in 70% of patients. At a cut-off stone diameter of >10.5 mm and CBD diameter of >12.5 mm, the AUC was 0.890 and 0.884, respectively, to predict failed clearance of CBD. On multivariate analysis, stone diameter ≥15 mm [odds ratio (OR) 16.97, 95% confidence interval (CI): 1.629-176.785], location of stones in hepatic ducts (OR 7.74, 95%CI: 2.041-29.332), presence of stricture distal to stone (OR 6.99, 95%CI: 1.402-34.726) and impacted stone (OR 21.61, 95%CI: 1.84-253.058) were independent predictors of failed bile duct clearance.
Conclusion: Stone size and location are independent predictors of failed bile duct clearance. The endoscopist should consider these factors while subjecting a patient to biliary ductal clearance to plan additional intervention.
Keywords: ERCP; CBD stone; gallstone disease; bile duct clearance; mechanical lithotripsy
RESUMO
Contexto: Cálculos do ducto biliar comum (CDC) são conhecidos por complicar 10-15% das doenças de cálculos biliares. A colangiopancreatografia retrógrada endoscópica (CPRE) é a modalidade terapêutica de escolha para a limpeza do CDC, mas pode falhar na sua remoção.
Objetivo: Este estudo prospectivo foi realizado para identificar os previsores de falha na limpeza do CDC com CPRE.
Métodos: Pacientes consecutivos com cálculos no ducto biliar submetidos a CPRE em um centro de atendimento terciário foram incluídos prospectivamente de outubro de 2020 a outubro de 2021. O principal resultado do estudo foi identificar e analisar fatores que poderiam prever a falha na limpeza completa do CDC.
Resultados: Um total de 120 pacientes (50,8% homens, idade média: 53,5 anos) foram incluídos na análise final. A limpeza bem-sucedida dos cálculos de CDC durante o procedimento inicial foi alcançada em 70% dos pacientes. Com um diâmetro de corte de cálculos >10,5 mm e de diâmetro de CDC de >12,5 mm, a AUC foi de 0,890 e 0,884, respectivamente, para prever a falha na limpeza do CDC. Na análise multivariada, diâmetro da cálculos ≥15 mm [razão de chances (OR) 16,97, intervalo de confiança de 95% (IC): 1,629-176,785], localização dos cálculos nos ductos hepáticos (OR 7,74, IC95%: 2,041-29,332), presença de estreitamento distal ao cálculo (OR 6,99, IC95%: 1,402-34,726) e cálculo impactado (OR 21,61, IC95%: 1,84-253,058) foram previsores independentes de falha na limpeza do ducto biliar.
Conclusão: O tamanho e a localização dos cálculos são previsores independentes de falha na limpeza do ducto biliar. O endoscopista deve considerar esses fatores ao submeter um paciente à limpeza ductal biliar para planejar intervenção adicional.
Palavras-chave: CPRE; cálculo de ducto biliar comum; doença de cálculos biliares; limpeza do ducto biliar; litotripsia mecânica
HIGHLIGHTS
• Failure to clear bile duct stones in the index ERCP can be seen in 15-20% of cases, and identifying the factors associated with failure is important.
• A prospective analysis was conducted to identify and analyze the factors that could predict the failure of complete CBD clearance.
• The present study reported a successful clearance of CBD stones during the index procedure in only 70% of patients.
• A stone diameter ≥15 mm, location of stones in hepatic ducts, presence of stricture distal to stone, and impacted stone were independent predictors of failed bile duct clearance.
INTRODUCTION
Common bile duct (CBD) stones complicate 10-15% of gallstone diseases, the majority being cholesterol gallstones1. In Indian studies, most CBD stones are of cholesterol type in the North and pigmented stones in the South2. Endoscopic retrograde cholangiopancreatography (ERCP) is the procedure of choice for the extraction of CBD stones, with a success rate of 80-85% during index procedure3. However, certain factors cause hindrance to CBD clearance during index procedure, resulting in repeated attempts for clearance or surgical exploration.
These factors can be related to the stone itself, like size, shape, location, or impaction, or the anatomy of the biliary tract, like CBD stricture, distal CBD angulation, stone/CBD ratio, or periampullary diverticulum4. Identifying these factors before the endoscopic intervention helps the team to allocate additional resources and personnel for clearance of ‘difficult’ stones viz, mechanical lithotripsy, cholangioscopy assisted lithotripsy, or ESWL5. It can also help prognosticate the patients regarding the achievement of CBD clearance, cost of treatment, and need for surgical CBD exploration.
The present study aimed to prospectively evaluate the factors that can predict the failure of index ERCP in complete clearance of the biliary system in patients presenting with symptomatic CBD stones. The findings of this research can help gain a better understanding of the risk factors associated with difficult CBD stone extraction and develop better future strategies for managing such cases.
METHODS
Study design and patient selection
This was a single-center, prospective observational study conducted at a tertiary health care center in South India. All consecutive patients diagnosed with bile duct stones from October 2020 to October 2021 and undergoing their index ERCP procedure were recruited. The diagnosis of bile duct stone was based on radiologic and endosonological findings. The study was conducted as per the Declaration of Helsinki after approval of the Institutional Ethical Committee (EC/NIMS/2642/2020).
Exclusion criteria
The following patients were excluded from the study: (i) prior attempts of bile duct stone extraction by ERCP, (ii) extracorporeal shock wave lithotripsy (ESWL) prior to the procedure, (iii) failed cannulation of CBD, (iv) uncorrected coagulopathy or patients on antithrombotics or anticoagulants within previous five days, and (v) pregnant women.
Treatment protocol
Preprocedural work-up included complete blood cell count, liver function tests, serum electrolytes, and coagulation studies. After taking informed consent, the procedure was performed with the patient in the prone or left lateral position. All procedures were done under moderate sedation or general anesthesia, depending upon the patient’s general condition, with continuous vital monitoring. ERCP was performed using a side-viewing duodenoscope (TJF-150, Olympus Optical Co., Tokyo, Japan) by two endoscopists with experience of at least 300 ERCPs prior to these procedures. Guide-wire-assisted cannulation of the common bile duct (CBD) was done, followed by a contrast injection delineating the location of the stone and associated strictures. Sphincterotomy was performed after a cholangiogram. In case of failure of cannulation using sphincterotome, needle knife sphincterotomy was performed. Stones in the biliary system were extracted with a 12-15 mm extraction balloon after sphincterotomy. In case of any stricture distal to the stone, balloon dilation with 6- or 8-mm balloons was performed prior to extraction. In case of stone extraction failure, sphincteroplasty was performed with a CRE balloon ranging from a diameter of 10 to 15 mm based on the size of the stone and bile duct. After the failure of the above procedures, a mechanical lithotripter was used to fragment the stones into smaller pieces. Finally, the contrast was injected into the CBD via the balloon catheter. The balloon was pulled out of the CBD and into the duodenum to confirm biliary clearance. Double pigtail plastic biliary stents of sizes ranging from 8.5 to 10 Fr. and lengths ranging from 8 to 10 cm (Cook Medical, USA) were placed based on cholangiogram findings.
Study outcomes and statistical analysis
The primary outcome of the study was complete CBD clearance, as visualized on the cholangiogram. Secondary outcomes included analysis of predictors of failure of stone clearance.
Continuous variables were expressed as mean (± standard deviation) or median (range) based on the normality test. Categorical variables were expressed as numbers and percentages. Pearson’s chi-square test was used to test the significance of factors affecting the clearance of CBD. Factors found to be significant in univariate analysis were entered into multivariate logistic regression analysis. A comparison of the predictive ability of factors affecting the clearance of bile duct stones was made using the area under the receiver operating characteristic (AUROC) curve. SPSS statistical package, version 24.0 statistical software, was used for statistical analyses.
RESULTS
Patient selection and baseline characteristics
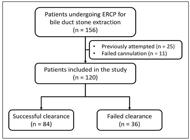
Over the study period, a total of 156 cases underwent ERCP for CBD stone extraction. Figure 1 shows the study flowchart for the patient selection process. The present study comprised 120 subjects, of which 61 were males, and 59 were females, with a M:F ratio of ~1:1. The population’s median age was 53.5 years (range: 22-85). The median size of stone and CBD were 10 mm (range: 6-25) and 11 mm (range: 6-28), respectively, with the number of stones ranging from 1 to 8. Ten percent (12/120) of the patients had a prior cholecystectomy. Jaundice was present in 30.8% (37/120) cases, and 17.5% (21/120) presented with features of acute cholangitis.
Predictors of incomplete biliary clearance on index ERCP
Successful clearance of CBD stones during the index procedure was achieved in 70% of patients. Table 1 compares the difference in parameters between patients with and without bile duct clearance at index ERCP. Proportions of patients with stone diameter ≥15 mm, CBD diameter ≥15 mm, location of stones in hepatic ducts, presence of stricture distal to stone, and impacted stone were higher in patients who failed biliary clearance.
For stone diameter, AUC was 0.890 (0.831-0.950) at a cut-off of >10.5 mm with a sensitivity of 88.9% and specificity of 76.2% to predict failed clearance of CBD. Similarly, for CBD diameter, AUC was 0.884 (0.825-0.943) at a cut-off of >12.5 mm with a sensitivity of 86.1% and specificity of 77.4% to predict failed clearance of CBD (Figure 2).

Receiver operating characteristic curve for stone diameter and bile duct diameter in predicting failure of stone clearance during ERCP.
A multivariable model was generated to analyze factors affecting the clearance of CBD during index ERCP. The model included stone diameter ≥15 mm, CBD diameter ≥15 mm, location of stones in hepatic ducts, presence of stricture distal to stone, and impacted stone (Table 2). Among these parameters, except for CBD diameter, all the above were significant factors that negatively impacted the clearance of bile duct stones during index ERCP.
DISCUSSION
Endoscopic management of bile duct stones aims to achieve complete CBD clearance. However, this may not be achieved in all cases, requiring additional interventional techniques such as endoscopic papillary large balloon dilatation (EPLBD), mechanical lithotripsy, and cholangioscopy-assisted lithotripsy. Multiple factors can help predict the failure of ERCP in clearing bile duct stones. The present study comprised 120 subjects undergoing their first ERCP procedure for bile duct stones, achieving successful clearance in 70% of cases. Significant factors that negatively impacted the success of ERCP in clearing bile duct stones during index procedure were stone diameter ≥15 mm, CBD diameter ≥15 mm, location of stones in hepatic ducts, presence of stricture distal to stone, and impacted stone on univariate analysis. On a multivariate logistic regression analysis, except for CBD diameter, all the above were significant factors that negatively impacted the clearance of bile duct stones during index ERCP.
In literature, ERCP with stone extraction has 80-85% success rates in treating CBD stones. However, in the study by Sabbah et al., CBD clearance by first-line techniques was achieved in 61.9% of the cases6. In the present study, only 70% of the patients could achieve CBD clearance. The low success rate in our study can be explained by the fact that our center, a tertiary care hospital, is a referral center for complex stone cases from primary and secondary care centers. Hence, Also, the lack of cholangioscopy-assisted lithotripsy may have led to a lower clearance rate.
According to previous studies6-10, the patient’s age was considered a significant factor affecting the clearance of CBD stones during ERCP, and older patients had increased failure rates. In contrast to the previous studies, the age (P=0.771) and sex (P=0.905) of the patients had no significant effect on the clearance of bile duct stones during ERCP in our study.
In a previous study by Garcia et al., a CBD diameter ≥15 mm was a significant predictor of failure of CBD clearance at index ERCP11. Subsequently, two other studies reported CBD diameter as a significant predictor6,8. In the present study, a CBD diameter of >12.5 mm was associated with a sensitivity and specificity of 86.1% and 77.4%, respectively, to predict failed clearance of CBD. However, CBD diameter did not reach statistical significance in a multivariate analysis in the present study. Hence, it was not an independent predictor of bile duct clearance but was considered secondary to the presence of large CBD stones.
Limited sphincterotomy combined with endoscopic papillary large-balloon dilation (EPLBD) is the first-line approach for removing difficult common bile duct stones12. Mechanical lithotripsy (ML) is the simplest method for fragmenting large CBD stones13. Both are additional intervention techniques for managing difficult CBD stones. In the present study, the use of these additional interventional techniques did not significantly affect the clearance of difficult stones (P=0.241 for ML and 0.285 for EPLBD). Balloon and basket catheters are comparable in efficacy and safety for common bile duct stone removal. Two multicenter RCTs have compared the efficacy of balloon vs basket catheters for extracting CBD stones sized ≤10 mm or <11 mm after endoscopic sphincterotomy14,15. In one RCT of 158 patients, the balloon catheter achieved a higher clearance rate than the basket catheter (92.3% vs 80.0%)14. The other RCT of 184 patients reported similar efficacies for basket and balloon catheters for stone extraction, but a stone diameter of <6 mm was independently associated with failed stone removal within 10 minutes using a basket catheter because of the inability to grasp the stone with the basket15. In the present study, the use of either balloon or basket catheters was comparable in extracting bile duct stones, and there was no statistically significant difference affecting the clearance of bile duct stones (P=0.178).
Two studies reported the presence of periampullary diverticulum as a significant factor contributing to failed ERCP on univariate analysis but not on multivariate analysis9,10. In the study by Sabbah et al., the presence of a periampullary diverticulum was a significant factor affecting the clearance of CBD in both univariate and multivariate analysis6. However, our study did not find any statistical significance between the presence of a periampullary diverticulum and the failure of CBD clearance (P-value=0.673). Hence, the presence of a periampullary diverticulum may be considered a difficult factor in the cannulation of CBD rather than stone extraction.
Multiple stone-related factors have been evaluated previously for predicting failed biliary clearance. Faceted stones are difficult to clear from CBD. According to previous studies, the number of stones in the bile ducts was considered a significant factor affecting the success of ERCP7,10,16. Also, the location of stones in the intrahepatic ducts poses technical challenges in achieving ERCP success17. In the present study, neither the number of stones nor their shape predicted the success of ERCP. However, stones located in the common hepatic or intrahepatic ducts significantly affected the clearance of bile ducts on both univariate and multivariate analysis (OR=7.74, 95%CI: 2.041-29.332). Thus, size and location are the two most important stone-related factors for predicting failed biliary clearance.
To the best of our knowledge, this is the first study from India on the technical challenges encountered with the endoscopic removal of CBD stones. Despite this, there were multiple limitations to the present study. The study’s major limitation was that patients not achieving clearance of bile duct stones during index ERCP were not subsequently followed to assess the clearance rate in subsequent procedures. Cholangioscopy-assisted lithotripsy was not used for managing difficult CBD stones
To conclude, stone diameter ≥15 mm, intrahepatic location, presence of distal stricture, and impacted stone are independent predictors of failure of ERCP clearing bile duct stones during the index procedure. For patients at high risk of failure of CBD clearance during index ERCP, the treating team and the patient should be prepared for second-line interventions like EPLBD or mechanical lithotripsy. Conversely, such patients can be referred to centers with facilities for cholangioscopy-assisted lithotripsy to avoid repeated endoscopic sessions.
REFERENCES
- 1 Soltan HM, Kow L, Toouli J. A simple scoring system for predicting bile duct stones in patients with cholelithiasis. J Gastrointest Surg. 2001;5:434-7.
- 2 Tandon RK. Prevalence and type of biliary stones in India. World J Gastroenterol. 2000;6:4-5.
- 3 David QH, Wang Nezam H. Afdhal. Gall stone disease; sleisenger and fordtrans gastrointestinal and liver diseases, 11th Ed. 2021; 65;1032-33.
- 4 Cheng CL, Tsou YK, Lin CH, Tang JH, Hung CF, Sung KF, et al. Poorly expandable common bile duct with stones on endoscopic retrograde cholangiography. World J Gastroenterol . 2012;18:2396-401.
- 5 Aljebreen AM, Alharbi OR, Azzam N, Almadi MA. Efficacy of spyglass-guided electrohydraulic lithotripsy in difficult bile duct stones. Saudi J Gastroenterol. 2014; 20:366-70.
- 6 Sabbah M, Nakhli A, Bellil N, Ouakaa A, Bibani N, Trad D, et al., Predictors of failure of endoscopic retrograde pancreato cholangiography during common bile duct stones. Heliyon. 2020;6:e05515.
- 7 Almadi MA, Eltayeb M, Thaniah S, Alrashed F, Aljebreen MA, Alharbi OR, et al. Predictors of failure of endoscopic retrograde cholangiography in clearing bile duct stone on the initial procedure. Saudi J Gastroenterol . 2019;25:132-8.
- 8 Ödemiş B, Kuzu UB, Öztaş E, Saygılı F, Suna N, Coskun O, et al., Endoscopic Management of the Difficult Bile Duct Stones: A Single Tertiary Center Experience. Gastroenterol Res Pract. 2016;2016:8749583.
- 9 Kim HJ, Choi HS, Park JH Park DI, Cho YK, Sohn CI, et al. Factors influencing the technical difficulty of endoscopic clearance of bile duct stones. Gastrointest Endosc. 2007;66:1154-60.
- 10 Christoforidis E, Vasiliadis K, Tsalis K, Patridas D, Blouhos K, Pramateftakis MG, et al. Factors significantly contributing to a failed conventional endoscopic stone clearance in patients with “difficult” choledocholithiasis: a single-center experience. Diagn Ther Endosc. 2014;2014:861689.
- 11 Ramírez García J. Factors related to therapeutic failure in the extraction of bile duct stones for endoscopic retrograde colangiopancreatography ERCP. Rev Gastroenterol Peru. 2011;31:330-4.
- 12 Rouquette O, Bommelaer G, Abergel A, Poincloux L. Large balloon dilation post endoscopic sphincterotomy in removal of difficult common bile duct stones: a literature review. World J Gastroenterol . 2014;20:7760-6.
- 13 Chang WH, Chu CH, Wang TE, Chen MJ, Lin CC. Outcome of simple use of mechanical lithotripsy of difficult common bile duct stones. World J Gastroenterol . 2005;11:593-6.
- 14 Ishiwatari H, Kawakami H, Hisai H, Yane K, Onodera M, Eto K, et al; Hokkaido Interventional EUS/ERCP Study (HONEST) Group. Balloon catheter versus basket catheter for endoscopic bile duct stone extraction: a multicenter randomized trial. Endoscopy. 2016;48:350-7.
- 15 Ozawa N, Yasuda I, Doi S, Iwashita T, Shimizu M, Mukai T, et al. Prospective randomized study of endoscopic biliary stone extraction using either a basket or a balloon catheter: the BasketBall study. J Gastroenterol. 2017;52:623-30.
- 16 Williams EJ, Ogollah R, Thomas P, Logan RF, Martin D, Wilkinson ML, et al. What predicts failed cannulation and therapy at ERCP? Results of a large-scale multicenter analysis. Endoscopy. 2012;44:674-83.
- 17 Williams E, Beckingham I, El Sayed G, Gurusamy K, Sturgess R, Webster G, et al. Updated guideline on the management of common bile duct stones (CBDS). Gut. 2017;66:765-82.
Publication Dates
-
Publication in this collection
04 Mar 2024 -
Date of issue
2024
History
-
Received
27 July 2023 -
Accepted
31 Oct 2023


