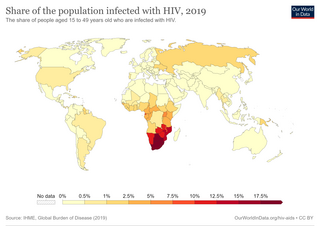
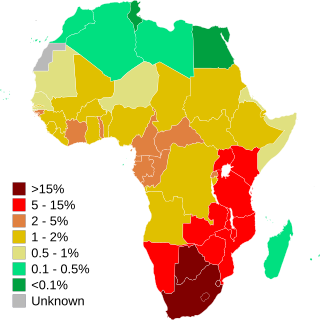
Prevalence of HIV/AIDS in Africa, total (% of population ages 15–49), in 2021 (World Bank)
HIV/AIDS originated in the early 20th century and remains a significant public health challenge, particularly in Africa. Although the continent constitutes about 17% of the world's population,[1] it bears a disproportionate burden of the epidemic. As of 2023, around 25.6 million people in sub-Saharan Africa were living with HIV, accounting for over two-thirds of the global total.[2] The majority of new infections and AIDS-related deaths occur in Eastern and Southern Africa, which house approximately 55% of the global HIV-positive population.[3]
In regions such as Southern Africa, the epidemic is particularly severe. Countries including Botswana, Lesotho, Malawi, Mozambique, Namibia, South Africa, Eswatini, Zambia, and Zimbabwe exhibit adult prevalence rates exceeding 10%.[4] This has significantly affected life expectancy, with reductions of up to 20 years in the most impacted areas.[5] By contrast, North Africa, West Africa, and the Horn of Africa report significantly lower prevalence rates, attributed to differing cultural practices and reduced engagement in high-risk behaviors.[6] Efforts to combat the epidemic have focused on multiple strategies, including the widespread distribution of antiretroviral therapy (ART), which has substantially improved the quality of life and reduced mortality for those living with HIV.[7] Between 2010 and 2020, AIDS-related deaths declined by 43% in sub-Saharan Africa due to increased access to ART and prevention of mother-to-child transmission programs.[8] However, challenges persist, including stigma, insufficient healthcare infrastructure, and funding constraints.
Despite progress, gender inequalities exacerbate the epidemic's impact, with young women in sub-Saharan Africa experiencing HIV infection rates three times higher than their male counterparts.[11] Addressing socio-economic factors and enhancing HIV/AIDS education among at-risk populations remain vital components of comprehensive intervention strategies.
Overview
In a 2019 research article titled "The Impact of HIV & AIDS in Africa", the charitable organization AVERT wrote:
HIV ... has caused immense human suffering in the continent. The most obvious effect ... has been illness and death, but the impact ... has ... not been confined to the health sector; households, schools, workplaces and economies have also been badly affected. ...
In sub-Saharan Africa, people with HIV-related diseases occupy more than half of all hospital beds. ... [L]arge numbers of healthcare professionals are being directly affected.... Botswana, for example, lost 17% of its healthcare workforce due to AIDS between 1999 and 2005.
... The toll of HIV and AIDS on households can be very severe. ... [I]t is often the poorest sectors of society that are most vulnerable.... In many cases, ... AIDS causes the household to dissolve, as parents die and children are sent to relatives for care and upbringing. ... Much happens before this dissolution takes place: AIDS strips families of their assets and income earners, further impoverishing the poor. ...
The ... epidemic adds to food insecurity in many areas, as agricultural work is neglected or abandoned due to household illness. ...
Almost invariably, the burden of coping rests with women. Upon a family member becoming ill, the role of women as carers, income-earners and housekeepers is stepped up. They are often forced to step into roles outside their homes as well. ...
Older people are also heavily affected by the epidemic; many have to care for their sick children and are often left to look after orphaned grandchildren. ...
It is hard to overemphasise the trauma and hardship that children ... are forced to bear. ... As parents and family members become ill, children take on more responsibility to earn an income, produce food, and care for family members. ... [M]ore children have been orphaned by AIDS in Africa than anywhere else. Many children are now raised by their extended families and some are even left on their own in child-headed households. ...
HIV and AIDS are having a devastating effect on the already inadequate supply of teachers in African countries.... The illness or death of teachers is especially devastating in rural areas where schools depend heavily on one or two teachers. ... [I]n Tanzania[,] for example[,] ... in 2006 it was estimated that around 45,000 additional teachers were needed to make up for those who had died or left work because of HIV....
AIDS damages businesses by squeezing productivity, adding costs, diverting productive resources, and depleting skills. ... Also, as the impact of the epidemic on households grows more severe, market demand for products and services can fall. ... In many countries of sub-Saharan Africa, AIDS is erasing decades of progress in extending life expectancy. ... The biggest increase in deaths ... has been among adults aged between 20 and 49 years. This group now accounts for 60% of all deaths in sub-Saharan Africa.... AIDS is hitting adults in their most economically productive years and removing the very people who could be responding to the crisis. ...
As access to treatment is slowly expanded throughout the continent, millions of lives are being extended and hope is being given to people who previously had none. Unfortunately though, the majority of people in need of treatment are still not receiving it, and campaigns to prevent new infections ... are lacking in many areas.[12]
The earliest known cases of human HIV infection were in western equatorial Africa, probably in southeastern Cameroon where groups of the central common chimpanzee live. "Phylogenetic analyses revealed that all HIV-1 strains known to infect humans, including HIV-1 groups M, N, and O, were closely related to just one of these SIV cpz lineages: that found in P. t. troglodytes [Pan troglodytes troglodytes i.e. the central chimpanzee]." It is suspected that the disease jumped to humans from butchering of chimpanzees for human consumption.[15][16]
Current hypotheses also include that, once the virus jumped from chimpanzees or other apes to humans, medical practices of the early 20th century helped HIV become established in human populations by 1930.[17] The virus likely moved from primates to humans when hunters came into contact with the blood of infected primates. The hunters then became infected with HIV and passed on the disease to other humans through bodily fluid contamination. This theory is known as the "Bushmeat theory".[18]
HIV made the leap from rural isolation to rapid urban transmission as a result of urbanization that occurred during the 20th century. There are many reasons why there is such a high prevalence of AIDS in Africa. One of the most formative explanations is the poverty that dramatically impacts the daily lives of Africans. The book, Ethics and AIDS in Africa: A Challenge to Our Thinking, describes how "Poverty has accompanying side-effects, such as prostitution (i.e. the need to sell sex for survival), poor living conditions, education, health and health care, that are major contributing factors to the current spread of HIV/AIDS."[19]
Researchers believe HIV was gradually spread by river travel. All the rivers in Cameroon run into the Sangha River, which joins the Congo River running past Kinshasa in the Democratic Republic of the Congo. Trade along the rivers could have spread the virus, which built up slowly in the human population. By the 1960s, about 2,000 people in Africa may have had HIV,[16] including people in Kinshasa whose tissue samples from 1959 and 1960 have been preserved and studied retrospectively.[20] The first epidemic of HIV/AIDS is believed to have occurred in Kinshasa in the 1970s, signaled by a surge in opportunistic infections such as cryptococcal meningitis, Kaposi's sarcoma, tuberculosis, and pneumonia.[21][22]
History
Prevalence of HIV/AIDS in Africa over the years
Acquired immunodeficiency syndrome (AIDS) is a fatal disease caused by the slow-acting human immunodeficiency virus (HIV). The virus multiplies in the body until it causes immune system damage, leading to diseases of the AIDS syndrome. HIV emerged in Africa in the 1960s and spread to the United States and Europe the following decade. In the 1980s it spread across the globe until it became a pandemic. Some areas of the world were already significantly impacted by AIDS, while in others the epidemic was just beginning. The virus is transmitted by bodily fluid contact including the exchange of sexual fluids, by blood, from mother to child in the womb, and during delivery or breastfeeding. AIDS first was identified in the United States and France in 1981, principally among homosexual men. Then in 1982 and 1983, heterosexual Africans also were diagnosed.[23]
In the late 1980s, international development agencies regarded AIDS control as a technical medical problem rather than one involving all areas of economic and social life. Because public health authorities perceived AIDS to be an urban phenomenon associated with prostitution, they believed that the majority of Africans who lived in "traditional" rural areas would be spared. They believed that the heterosexual epidemic could be contained by focusing prevention efforts on persuading the so-called core transmitters—people such as sex workers and truck drivers, known to have multiple sex partners—to use condoms. These factors hindered prevention campaigns in many countries for more than a decade.[23]
Prevalence of HIV/AIDS in Africa over the years
Although many governments in Sub-Saharan Africa denied that there was a problem for years, they have now begun to work toward solutions.[24]
AIDS was at first considered a disease of gay men and people suffering from drug addiction, but in Africa it took off among the general population. As a result, those involved in the fight against HIV began to emphasize aspects such as preventing transmission from mother to child, or the relationship between HIV and poverty, inequality of the sexes, and so on, rather than emphasizing the need to prevent transmission by unsafe sexual practices or drug injection. This change in emphasis resulted in more funding, but was not effective in preventing a drastic rise in HIV prevalence.[25]
According to the Joint United Nations Program on HIV/AIDS (UNAIDS), the number of HIV positive people in Africa receiving anti-retroviral treatment rose from 1 million to 7.1 million between 2005 and 2012, an 805% increase. Almost 1 million of those patients were treated in 2012.[27] The number of HIV positive people in South Africa who received such treatment in 2011 was 75.2 percent higher than the number in 2009.[13]
Additionally, the number of AIDS-related deaths in 2011 in both Africa as a whole and Sub-Saharan Africa alone was 32 percent less than the number in 2005.[27][13] The number of new HIV infections in Africa in 2011 was also 33 percent less than the number in 2001, with a "24% reduction in new infections among children from 2009 to 2011".[27] In Sub-Saharan Africa, new HIV positive cases over the same period declined by 25%.[13] According to UNAIDS, these successes have resulted from "strong leadership and shared responsibility in Africa and among the global community".[28]
Prevention of HIV infections
AIDS awareness sign in central Dar es Salaam, Tanzania
Public education initiatives
Numerous public education initiatives have been launched to curb the spread of HIV in Africa.[29]
Many activists have drawn attention to stigmatization of those testing as HIV positive. This is due to many factors such as a lack of understanding of the disease, lack of access to treatment, the media, knowing that AIDS is incurable, and prejudices brought on by a cultures beliefs.[30] "When HIV/AIDS became a global disease, Some African leaders played ostrich and said that it was a gay disease found only in the West and Africans did not have to worry because there were no gays and lesbians in Africa".[31] Africans were blind to the already huge epidemic that was infesting their communities. The belief that only homosexuals could contract the diseases was later debunked as the number of heterosexual couples living with HIV increased. Unfortunately there were other rumors being spread by elders in Cameroon. These "elders speculated that HIV/AIDS was a sexually transmitted disease passed on from Fulani women only to non-Fulani men who had sexual contact with them. They also claimed if a man was infected as a result of having sexual contact with a Fulani woman, only a Fulani healer could treat him".[32] This communal belief is shared by many other African cultures who believe that HIV and AIDS originated from women. Because of this belief that men can only get HIV from women many "women are not free to speak of their HIV status to their partners for fear of violence".[30] In general HIV carries a negative stigma in Sub-Saharan Africa. Unfortunately This stigma makes it very challenging for Sub-Saharan Africans to share that they have HIV because they are afraid of being an outcast from their friends and family. In every Sub-Saharan community HIV is seen as the bringer of death. The common belief is that once you have HIV you are destined to die. People seclude themselves based on these beliefs. They do not tell their family and live with guilt and fear because of HIV. However, there is a way to treat HIV and AIDS the problem is that many are just not aware of how HIV is spread or what effects it has on the body. "80.8% of participants would not sleep in the same room as someone who was HIV positive, while 94.5% would not talk to someone who was HIV positive".[30]
Social stigma plays a significant role in the state of HIV and AIDS infection in Africa. "In a normatively HIV/AIDS-stigmatizing Sub Saharan African communities, this suspicion of one's status by others is also applicable to individuals who are not HIV positive, but who may wish to utilize healthcare services for preventive purposes. This group of individuals under fear of suspicion may avoid being mistakenly identified as stigmatized by simply avoiding HARHS utilization." (151)[19]
"At the individual level, persons living with HIV/AIDS in Sub-Saharan Africa likely want to conceal their stigmatized identities whenever possible in order to gain these rewards associated with having a 'normal' identity. The rewards of being considered normal' in the context of high-HIV-prevalence Sub-Saharan Africa are varied and great... such rewards for which there is empirical support in this context include perceived sexual freedom, avoidance of discrimination, avoidance of community or family rejection, avoidance of losing one's job or residence, and avoidance of losing one's sexual partners. Other potential rewards of being considered normal include avoidance of being associated with promiscuity or prostitution, avoidance of emotional, social and physical isolation and avoidance of being blamed for others' illness" (150).[19]
rights-based, evidence-informed, and community-owned programs that use a mix of biomedical, behavioral, and structural interventions, prioritized to meet the current HIV prevention needs of particular individuals and communities, so as to have the greatest sustained impact on reducing new infections. Well-designed programs are carefully tailored to national and local needs and conditions; focus resources on the mix of programmatic and policy actions required to address both immediate risks and underlying vulnerability; and are thoughtfully planned and managed to operate synergistically and consistently on multiple levels (e.g. individual, relationship, community, society) and over an adequate period of time. Using different prevention strategies in combination is not a new idea combination approaches have been used effectively to generate sharp, sustained reductions in new HIV infections in diverse settings. Combination prevention reflects common sense, yet it is striking how seldom the approach has been put into practice. Prevention efforts to date have overwhelmingly focused on reducing individual risk, with fewer efforts made to address societal factors that increase vulnerability to HIV. UNAIDS' combination prevention framework puts structural interventions—including programs to promote human rights, to remove punitive laws that block the AIDS response, and to combat gender inequality and HIV related stigma and discrimination—at the center of the HIV prevention agenda.[33]
"It is the consensus in the HIV scientific community that abstinence, be faithful, use a condom [(ABC)] principles are vital guides for public health intervention, but are better bundled with biomedical prevention approaches; lone behavioral change approaches are not likely to stop the global pandemic."[34]Uganda has replaced its ABC strategy with a combination prevention program because of an increase in the annual HIV infection rate. Most new infections were coming from people in long-term relationships who had multiple sexual partners.[35]
Abstinence, be faithful, use a condom
The abstinence, be faithful, use a condom (ABC) strategy to prevent HIV infection promotes safer sexual behavior and emphasizes the need for fidelity, fewer sexual partners, and a later age of sexual debut. The implementation of ABC differs among those who use it. For example, the President's Emergency Plan for AIDS Relief has focused more on abstinence and fidelity than condoms[36] while Uganda has had a more balanced approach to the three elements.[37]
Much of the ABC message was getting through, but it was not making much of a difference. A program called Total Community Mobilization sent 450 AIDS counselors door-to-door, giving prevention advice, urging HIV testing and referring infected people to treatment. People who had talked to the counselors were twice as likely to mention abstinence and three times as likely to mention condom use when asked to describe ways to avoid infection. However, they were no more likely than the uncounseled to mention being faithful as a good strategy. The people who had been counseled were also twice as likely to have been tested for HIV in the previous year, and to have discussed that possibility with a sex partner. However, they were just as likely to have a partner outside marriage as the people who had not gotten a visit from a counselor, and they were no more likely to be using a condom in those liaisons.[38]
There was a somewhat different result in a study of young Nigerians, ages 15 to 24, most unmarried, living in the city and working in semiskilled jobs. People in specific neighborhoods were counseled with an ABC message as part of a seven-year project funded by the [[United States Agency for International Development [U.S. Agency for International Development] and its British counterpart. The uncounseled group showed no increase in condom use—it stayed about 55 percent. In the counseled group, however, condom use by women in their last nonmarital sexual encounter rose from 54 percent to 69 percent. For men, it rose from 64 percent to 75 percent. Stigmatizing attitudes appeared to be less common among the counseled group. But "We did not see a reduction in the number of partners," said Godspower Omoregie, the researcher from Abuja who presented the findings.[38]
A survey of 1,400 Kenyan teenagers found a fair amount of confusion about ABC's messages. Half of the teenagers could correctly define abstinence and explain why it was important. Only 23 percent could explain what being faithful meant and why it was important. Some thought it meant being honest, and some thought it meant having faith in the fidelity of one's partner. Only 13 percent could correctly explain the importance of a condom in preventing HIV infection. About half spontaneously offered negative opinions about condoms, saying they were unreliable, immoral and, in some cases, were designed to let HIV be transmitted.[38]
An estimated value of about 300,000 people(All ages) have been infected with the HIV virus. This is prevalent and highest in the Eastern Region of Ghana and lowest in the Northern Regions of the country. As part of national efforts to control the wide spread of the HIV virus, the ABC approach is a popular strategy employed for HIV prevention in the country. The virus is higher among women than among men in all age groups with estimates of 56 percent among females and 44 percent among male. Sexual transmission remains the major mode of HIV transmission in Ghana but other approaches such as Information Education and Communication (IEC) and Behavior Change Communication (BCC) are all been used for the course of the virus prevention.[39]
Eswatini in 2010 announced that it was abandoning the ABC strategy because it was a dismal failure in preventing the spread of HIV. "If you look at the increase of HIV in the country while we've been applying the ABC concept all these years, then it is evident that ABC is not the answer," said Dr. Derek von Wissell, Director of the National Emergency Response Council on HIV/AIDS.[40]
In 2011, the Botswana Ministry of Education introduced new HIV/AIDS educational technology in local schools. The TeachAids prevention software, developed at Stanford University, was distributed to every primary, secondary, and tertiary educational institution in the country, reaching all learners from 6 to 24 years of age nationwide.[42]
African Union's efforts
AIDS Watch Africa
During the Abuja African Union Summit on HIV/AIDS in April 2001, the heads of state and heads of government of Botswana, Ethiopia, Kenya, Mali, Nigeria, Rwanda, South Africa, and Uganda established the AIDS Watch Africa (AWA) advocacy platform. The initiative was formed to "accelerate efforts by Heads of State and Government to implement their commitments for the fight against HIV/AIDS, and to mobilize the required national and international resources."[43] In January 2012, AWA was revitalized to include all of Africa and its objectives were broadened to include malaria and tuberculosis.[44]
Roadmap on Shared Responsibility and Global Solidarity for AIDS, TB and Malaria Response in Africa
In 2012, the African Union adopted a Roadmap on Shared Responsibility and Global Solidarity for AIDS, TB and Malaria Response in Africa.[28] This Roadmap outlines a set of African-developed strategies to strengthen shared responsibility and international cooperation for achieving sustainable AIDS solutions in Africa by 2015. The solutions are organized around three strategic pillars: diversified financing; access to medicines; and enhanced health governance. The Roadmap defines goals, results and roles and responsibilities to hold stakeholders accountable for the realization of these solutions between 2012 and 2015.[45]
Preventing HIV transmission from pregnant women to children
High-risk behavioral patterns are largely responsible for the significantly greater spread of HIV/AIDS in Sub-Saharan Africa than in other parts of the world. Chief among these are the traditionally liberal attitudes espoused by many communities inhabiting the subcontinent toward multiple sexual partners and pre-marital and outside marriage sexual activity.[46][47] HIV transmission is most likely in the first few weeks after infection, and is therefore increased when people have more than one sexual partner in the same time period. In most of the developed world outside Africa, this means HIV transmission is high among prostitutes and other people who may have more than one sexual partner concurrently. Within the cultures of sub-Saharan Africa, it is relatively common for both men and women to be carrying on sexual relations with more than one person, which promotes HIV transmission.[25] This practice is known as concurrency, which Helen Epstein describes in her book, The Invisible Cure: Africa, the West, and the Fight against AIDS, in which her research into the sexual mores of Uganda revealed the high frequency with which men and women engage in concurrent sexual relationships.[48] In addition, in sub-Saharan Africa AIDS is the leading killer and a large reason for the high transmission rates is because of the lack of education provided to youth. When infected, most children die within one year because of the lack of treatment.[49] All demographic populations in Sub-Saharan Africa have been infected with HIV, from men to women, and from pregnant women to children. Rather than having more of a specific group infected, male or female, the ratio of men and women infected with HIV are quite similar. With the HIV infection, 77% of men, women, and children, develop AIDS, and die in Sub-Saharan Africa. In addition, "more than 90% of AIDS orphans and children [were] infected with HIV".[50]
Lack of money is an obvious challenge, although a great deal of aid is distributed throughout developing countries with high HIV/AIDS rates. For African countries with advanced medical facilities, patents on many drugs have hindered the ability to make low cost alternatives.[51]
Natural disasters and conflict are also major challenges, as the resulting economic problems people face can drive many young women and girls into patterns of sex work in order to ensure their livelihood or that of their family, or else to obtain safe passage, food, shelter or other resources.[52] Emergencies can also lead to greater exposure to HIV infection through new patterns of sex work. In Mozambique, an influx of humanitarian workers and transporters, such as truck drivers, attracted sex workers from outside the area.[52] Similarly, in the Turkana District of northern Kenya, drought led to a decrease in clients for local sex workers, prompting the sex workers to relax their condom use demands and search for new truck driver clients on main highways and in peri-urban settlements.[52]
Health industry
Sub-Saharan "Africans have always appreciated the importance of health care because good health is seen as necessary for the continuation and growth of their lineage".[53] Without proper health the culture will not be able to thrive and grow. Unfortunately, "health services in many countries are swamped by the need to care for increasing numbers of infected and sick people. Ameliorative drugs are too expensive for most victims, except for a very small number who are affluent".[53] The greatest number of sick people with the fewest doctors, Sub-Saharan Africa "has 11 percent of the world's population but carries 24 percent of the global disease burden. With less than 1 percent of global health expenditure and only 3 percent of the world's health workers".[citation needed]
Measuring an HIV patient's CD4 count at the Kyabugimbi Health Center in Uganda
When family members get sick with HIV or other sicknesses, family members often end up selling most of their belongings in order to provide health care for the individual. Medical facilities in many African countries are lacking. Many health care workers are also not available, in part due to lack of training by governments and in part due to the wooing of these workers by foreign medical organizations where there is a need for medical professionals.[54] Unfortunately, many individuals who get a medical degree end up leaving Sub-Saharan Africa to work abroad "either to escape instability or to practice where they have better working conditions and a higher salary".[55] Many low income communities are very far away from a hospital and they cannot afford to bus there or pay for medical attention once they arrive. "Healthcare in Africa differs widely, depending on the country and also the region – those living in urban areas are more likely to receive better healthcare services than those in rural or remote regions".[55] It is very common to just wait out a sickness or seek help from a neighbor or relative. Currently antiretroviral therapy is the closest to a cure. However, many hospitals lack enough antiretroviral drugs to treat everyone. This may be because most Sub-Saharan African countries invest "as little as 1-4 dollars per capita, [so] overseas aid is a major source of funding for healthcare".[55] Many overseas organizations are very hesitant to give antiretroviral drugs to Sub-Saharan Africa because they are expensive, which means that there is only so much they can give. Relying on other countries for help in general requires more paperwork and faith in another country very far away. Also, delivery of drugs and other aid takes many month and years to arrive in the hands of those that need help.[56]
Medical factors
Medical suspicion
An HIV/AIDS educational outreach session in Angola
There are high levels of medical suspicion throughout Africa, and there is evidence that such distrust may have a significant impact on the use of medical services.[57][58] The distrust of modern medicine is sometimes linked to theories of a "Western Plot"[59] of mass sterilization or population reduction, perhaps a consequence of several high-profile incidents involving western medical practitioners.[60]
Pharmaceutical industry
Africans are still fighting against unethical human experimentation and other practices of unfair treatment by the pharmaceutical industry.[61] Medical experimentation occurs in Africa on many medications, but once approved, access to the drug is difficult.[61]
South African scientists in a combined effort with American scientists from Gilead Sciences recently tested and found effective a tenofovir-based anti-retroviral vaginal gel that could be used as pre-exposure prophylaxis. Testing of this gel was conducted at the University of KwaZulu-Natal in Durban, South Africa.[62] The FDA in the US is in the process of reviewing the drug for approval for US use.[63][64] The AIDS/HIV epidemic has led to the rise in unethical medical experimentation in Africa.[61]
Since the epidemic is widespread, African governments sometimes relax their laws in order to get research conducted in their countries which they would otherwise not afford.[61] However, global organizations such as the Clinton Foundation, are working to reduce the cost of HIV/AIDS medications in Africa and elsewhere. For example, the philanthropist Inder Singh oversaw a program which reduced the cost of paediatric HIV/AIDS drugs by between 80 and 92 percent by working with manufacturers to reduce production and distribution costs.[65] Manufacturers often cite distribution and production difficulties in developing markets, which create a substantial barrier to entry.[56]
Political factors
Major African political leaders have denied the link between HIV and AIDS, favoring alternate theories.[66] The scientific community considers the evidence that HIV causes AIDS to be conclusive and rejects AIDS-denialist claims as pseudoscience based on conspiracy theories, faulty reasoning, cherry picking, and misrepresentation of mainly outdated scientific data.[67]
Subtype factor
Subtypes A and C are the most prevalent HIV subtypes in Africa, and subtype C is the most prominent in the world, accounting for about 50% of all HIV infections.[68][69] Despite this, the majority of HIV research has historically been focused on subtype B, which constitutes only 12% of infections, mostly in Europe.[70] Due to this lack of research, it is currently unclear whether or not subtype C has evolved factors for increased viral transmission compared to other HIV subtypes.[70]
Religious factors
Pressure from both Christian and Muslim religious leaders has resulted in the banning of a number of safe-sex campaigns, including condom promoting advertisements.[71]
Health care delivery
While there is currently no cure or vaccine for HIV/AIDS there are emerging treatments. It has been extensively discussed that antiretroviral drugs (ART) are crucial for preventing the acquiring of AIDS. AIDS is acquired at the final stage of the HIV virus, which can be completely averted. It is overwhelmingly possible to live with the virus and never acquire AIDS. The proper obedience to ART drugs can provide an infected person with a limitless future. ART drugs are key in preventing the diseases from progressing as well as ensuring the disease is well controlled, thus forbidding the disease from becoming resistant to the treatments.[72] In countries like Nigeria and the Central African Republic, a mere less than 25% of the population has access to the ART drugs.[73] Funds devoted to ART drug access were measured at $19.1 billion in 2013 in low and middle-income countries among the region, however the funds were short of the UNAIDS' previous resource needs estimates of $22–24 billion by 2015.[74]
Prevalence measures include everyone living with HIV and AIDS, and present a delayed representation of the epidemic by aggregating the HIV infections of many years. Incidence, in contrast, measures the number of new infections, usually over the previous year. There is no practical, reliable way to assess incidence in Sub-Saharan Africa. Prevalence in 15- to 24-year-old pregnant women attending antenatal clinics is sometimes used as an approximation. The test done to measure prevalence is a sero survey in which blood is tested for the presence of HIV.[citation needed]
Health units that conduct sero surveys rarely operate in remote rural communities, and the data collected also does not measure people who seek alternate healthcare. Extrapolating national data from antenatal surveys relies on assumptions which may not hold across all regions and at different stages in an epidemic.[citation needed]
Thus, there may be significant disparities between official figures and actual HIV prevalence in some countries.[citation needed]
A minority of scientists claim that as many as 40 percent of HIV infections in African adults may be caused by unsafe medical practices rather than by sexual activity.[75] The World Health Organization states that about 2.5 percent of HIV infections in Sub-Saharan Africa are caused by unsafe medical injection practices and the "overwhelming majority" by unprotected sex.[76]
Regional prevalence
In contrast to areas in North Africa and the Horn of Africa, traditional cultures and religions in Sub-Saharan Africa have generally exhibited a more liberal attitude to female out-of-marriage sexual activity. The latter includes practices such as multiple sexual partners and unprotected sex, high-risk cultural patterns that have been implicated in the much greater spread of HIV in the subcontinent.[47]
As with North Africa, the HIV infection rates in the Horn of Africa are quite low. This has been attributed to the Muslim nature of many of the local communities and adherence to Muslim norms regarding sexuality.[47]
Ethiopia's HIV prevalence rate has decreased from 3.6 percent in 2001 to 1.4 percent in 2011.[13] The number of new infections per year also has decreased from 130,000 in 2001 to 24,000 in 2011.[13]
Kenya, according to a 2008 report from the Joint United Nations Program on HIV/AIDS, had the third largest number of individuals in Sub-Saharan Africa living with HIV.[78] It also had the highest prevalence rate of any country outside of Southern Africa.[78] Kenya's HIV infection rate dropped from around 14 percent in the mid-1990s to 5 percent in 2006,[46] but rose again to 6.2 percent by 2011.[78] The number of newly infected people per year, however, decreased by almost 30 percent, from 140,000 in 2001 to 100,000 in 2011.[13]
Christian men and women also had a higher infection rate than their Muslim counterparts.[78] This discrepancy was especially visible among women, with Muslim women showing a rate of 2.8 percent versus 8.4 percent among Protestant women and 8 percent among Catholic women.[78] HIV was also more common among the wealthiest than among the poorest (7.2 percent versus 4.6 percent).[78]
Historically, HIV had been more prevalent in urban than rural areas, although the gap is closing rapidly.[78] Men in rural areas are now more likely to be HIV-infected (at 4.5 percent) than those in urban areas (at 3.7 percent).[78]
Between 2004 and 2008, the HIV incidence rate in Tanzania for ages 15–44 slowed to 3.37 per 1,000 person-years (4.42 for women and 2.36 for men).[79] The number of newly infected people per year increased slightly, from 140,000 in 2001 to 150,000 in 2011.[13] There were also significantly fewer HIV infections in Zanzibar, which in 2011 had a prevalence rate of 1.0 percent compared to 5.3 percent in mainland Tanzania.[80]
Uganda has registered a gradual decrease in its HIV rates from 10.6 percent in 1997, to a stabilized 6.5–7.2 percent since 2001.[46][47] This has been attributed to changing local behavioral patterns, with more respondents reporting greater use of contraceptives[81] and a two-year delay in first sexual activity as well as fewer people reporting casual sexual encounters and multiple partners.[47]
The number of newly infected people per year, however, has increased by over 50 percent, from 99,000 in 2001 to 150,000 in 2011.[13] More than 40 percent of new infections are among married couples, indicating widespread and increasing infidelity.[82] This increase has caused alarm. The director of the Centre for Disease Control – Uganda, Wuhib Tadesse, said in 2011 that,
for every person started on antiretroviral therapy, there are three new HIV infections[,] and this is unsustainable. We are very concerned. Complacence could be part of the problem. Young people nowadays no longer see people dying; they see people on ARVs but getting children. We need to re-examine our strategies.... Leaders at all levels are spending [more] time in workshops than in the communities to sensitive the people[,] and this must stop."[83]
Western Africa has moderate levels of infection of both HIV-1 and HIV-2. The onset of the HIV epidemic in the region began in 1985 with reported cases in Senegal,[84] Benin,[85] and Nigeria.[86] These were followed in 1986 by Côte d'Ivoire.[87] The first identification of HIV-2 occurred in Senegal by microbiologist Souleymane Mboup and his collaborators.[84]
HIV prevalence in western Africa is lowest in Senegal and highest in Nigeria, which has the second largest number of people living with HIV in Africa after South Africa. Nigeria's infection rate (number of patients relative to the entire population), however, is much lower (3.7 percent) compared to South Africa's (17.3 percent).[citation needed]
In Niger in 2011, the national HIV prevalence rate for ages 15–49 was 0.8 percent while for sex workers it was 36 percent.[13]
Graphs of life expectancy at birth for some Sub-Saharan countries showing the fall in the 1990s primarily due to the AIDS pandemic
In the mid-1980s, HIV and AIDS were virtually unheard of in southern Africa. However, it is now the worst-affected region in the world. Currently, Eswatini and Lesotho have the highest and second highest HIV prevalence rates in the world, respectively.[77] Of the nine southern African countries (Botswana, Lesotho, Malawi, Mozambique, Namibia, South Africa, Eswatini, Zambia, and Zimbabwe), four are estimated to have an infection rate of over 15 percent.[citation needed]
In Botswana, the number of newly infected people per year has declined by 67 percent, from 27,000 in 2001 to 9,000 in 2011. In Malawi, the decrease has been 54 percent, from 100,000 in 2001 to 46,000 in 2011. All but two of the other countries in this region have also recorded major decreases (Namibia, 62 percent; Zambia, 54 percent; Zimbabwe, 47 percent; South Africa, 38 percent; Eswatini, 32 percent). The number has remained virtually the same in Lesotho and Mozambique.[13]
Zimbabwe's first reported case of HIV was in 1985.[89]
There are widespread practices of sexual networking that involve multiple overlapping or concurrent sexual partners.[90] Men's sexual networks, in particular, tend to be quite extensive,[91][92] a fact that is tacitly accepted or even encouraged by many communities.[93] Along with having multiple sexual partners, unemployment and population displacements resulting from drought and conflict have contributed to the spread of HIV/AIDS.[93] According to Susser and Stein (2000), men refuse to use condoms during intercourse with girls or women performing sex work (p.1043–1044). The girls and women are in desperate need of money and do not have a choice. This leads to multiple sex partners, which increases the likelihood of their infection with HIV/AIDS.[94]
A 2008 study in Botswana, Namibia, and Eswatini found that intimate partner violence, extreme poverty, education, and partner income disparity explained almost all of the differences in HIV status among adults aged 15–29 years. Among young women with any one of these factors, the HIV rate increased from 7.7 percent with no factors to 17.1 percent. Approximately 26 percent of young women with any two factors were HIV positive, with 36 percent of those with any three factors and 39.3 percent of those with all four factors being HIV-positive.[95]
As of 2011, the HIV prevalence rate in Eswatini was the highest in the world at 26.0 percent of persons aged 15–49.[77] The United Nations Development Program wrote in 2005,
The immense scale of AIDS-related illness and deaths is weakening governance capacities for service delivery, with serious consequences on food security, economic growth[,] and human development. AIDS undermines the capacities of individuals, families, communities[,] and the state to fulfill their roles and responsibilities in society. If current trends are not reversed, the longer-term survival of Swaziland as a country will be seriously threatened.[96]
The HIV epidemic in Eswatini has reduced its life expectancy at birth to 49 for men and 51 for women (based on 2009 data).[97] Life expectancy at birth in 1990 was 59 for men and 62 for women.[98]
Based on 2011 data, Eswatini's crude death rate of 19.51 per 1,000 people per year was the third highest in the world, behind only Lesotho and Sierra Leone.[99] HIV/AIDS in 2002 caused 64 percent of all deaths in the country.[100]
Much of the deadliness of the epidemic in Sub-Saharan Africa is caused by a deadly synergy between HIV and tuberculosis, termed a "co-epidemic".[101] The two diseases have been "inextricably bound together" since the beginning of the HIV epidemic.[102] "Tuberculosis and HIV co-infections are associated with special diagnostic and therapeutic challenges and constitute an immense burden on healthcare systems of heavily infected countries like Ethiopia."[103] In many countries without adequate resources, the tuberculosis case rate has increased five to ten-fold since the identification of HIV.[102] Without proper treatment, an estimated 90 percent of persons living with HIV die within months after contracting tuberculosis.[101] The initiation of highly active antiretroviral therapy in persons coinfected with tuberculosis can cause an immune reconstitution inflammatory syndrome with a worsening, in some cases severe worsening, of tuberculosis infection and symptoms.[104]
Since 2004, however, tuberculosis-related deaths among people living with HIV have fallen by 28 percent in Sub-Saharan Africa, which is home to nearly 80 percent of the people worldwide who are living with both diseases.[13]
Country
Concurrent HIV/Tuberculosis infections, 2011 (cases per 100,000 population)[105]
Male circumcision reduces the risk of human immunodeficiency virus (HIV) transmission from HIV positive women to men in high risk populations.
The global pandemic of HIV/AIDS began in 1981, and is an ongoing worldwide public health issue. According to the World Health Organization (WHO), by 2023, HIV/AIDS had killed approximately 40.4 million people, and approximately 39 million people were infected with HIV globally. Of these, 29.8 million people (75%) are receiving antiretroviral treatment. There were about 630,000 deaths from HIV/AIDS in 2022. The 2015 Global Burden of Disease Study estimated that the global incidence of HIV infection peaked in 1997 at 3.3 million per year. Global incidence fell rapidly from 1997 to 2005, to about 2.6 million per year. Incidence of HIV has continued to fall, decreasing by 23% from 2010 to 2020, with progress dominated by decreases in Eastern Africa and Southern Africa. As of 2023, there are about 1.3 million new infections of HIV per year globally.
The Caribbean is the second-most affected region in the world in terms of HIV prevalence rates. Based on 2009 data, about 1.0 percent of the adult population is living with the disease, which is higher than any other region except Sub-Saharan Africa. Several factors influence this epidemic, including poverty, gender, sex tourism, and stigma. HIV incidence in the Caribbean declined 49% between 2001 and 2012. Different countries have employed a variety of responses to the disease, with a range of challenges and successes.
The very high rate of human immunodeficiency virus infection experienced in Uganda during the 1980s and early 1990s created an urgent need for people to know their HIV status. The only option available to them was offered by the National Blood Transfusion Service, which carries out routine HIV tests on all the blood that is donated for transfusion purposes. The great need for testing and counseling resulted in a group of local non-governmental organizations such as The AIDS Support Organisation, Uganda Red Cross, Nsambya Home Care, the National Blood Bank, the Uganda Virus Research Institute together with the Ministry of Health establishing the AIDS Information Centre in 1990. This organization worked to provide HIV testing and counseling services with the knowledge and consent of the client involved.
Since the first HIV/AIDS case in Laos was identified in 1990, the number of infections has continued to grow. In 2005, UNAIDS estimated that 3,700 people in Laos were living with HIV.
The Democratic Republic of the Congo was one of the first African countries to recognize HIV, registering cases of HIV among hospital patients as early as 1983.
Kenya has a severe, generalized HIV epidemic, but in recent years, the country has experienced a notable decline in HIV prevalence, attributed in part to significant behavioral change and increased access to ARV. Adult HIV prevalence is estimated to have fallen from 10 percent in the late 1990s to about 4.8 percent in 2017. Women face considerably higher risk of HIV infection than men but have longer life expectancies than men when on ART. The 7th edition of AIDS in Kenya reports an HIV prevalence rate of eight percent in adult women and four percent in adult men. Populations in Kenya that are especially at risk include injecting drug users and people in prostitution, whose prevalence rates are estimated at 53 percent and 27 percent, respectively. Men who have sex with men (MSM) are also at risk at a prevalence of 18.2%. Other groups also include discordant couples however successful ARV-treatment will prevent transmission. Other groups at risk are prison communities, uniformed forces, and truck drivers.
HIV/AIDS in Lesotho constitutes a very serious threat to Basotho and to Lesotho's economic development. Since its initial detection in 1986, HIV/AIDS has spread at alarming rates in Lesotho. In 2000, King Letsie III declared HIV/AIDS a natural disaster. According to the Joint United Nations Programme on HIV/AIDS (UNAIDS) in 2016, Lesotho's adult prevalence rate of 25% is the second highest in the world, following Eswatini.
HIV/AIDS in Eswatini was first reported in 1986 but has since reached epidemic proportions. As of 2016, Eswatini had the highest prevalence of HIV among adults aged 15 to 49 in the world (27.2%).
HIV and AIDS is a major public health issue in Zimbabwe. The country is reported to hold one of the largest recorded numbers of cases in Sub-Saharan Africa. According to reports, the virus has been present in the country since roughly 40 years ago. However, evidence suggests that the spread of the virus may have occurred earlier. In recent years, the government has agreed to take action and implement treatment target strategies in order to address the prevalence of cases in the epidemic. Notable progress has been made as increasingly more individuals are being made aware of their HIV/AIDS status, receiving treatment, and reporting high rates of viral suppression. As a result of this, country progress reports show that the epidemic is on the decline and is beginning to reach a plateau. International organizations and the national government have connected this impact to the result of increased condom usage in the population, a reduced number of sexual partners, as well as an increased knowledge and support system through successful implementation of treatment strategies by the government. Vulnerable populations disproportionately impacted by HIV/AIDS in Zimbabwe include women and children, sex workers, and the LGBTQ+ population.
HIV/AIDS in Jordan is characterized by a low prevalence rate compared to other regions, but the situation remains a concern due to potential for increase and the social and economic consequences that could result. As of 2007, the UNAIDS estimated that there were approximately 380 people living with HIV/AIDS (PLWHA) in Jordan. Despite the relatively low numbers, the country faces challenges in addressing the epidemic, including inadequate surveillance systems, limited adoption of preventive practices, and persistent stigma and discrimination against PLWHA.
Since HIV/AIDS was first reported in Thailand in 1984, 1,115,415 adults had been infected as of 2008, with 585,830 having died since 1984. 532,522 Thais were living with HIV/AIDS in 2008. In 2009 the adult prevalence of HIV was 1.3%. As of 2016, Thailand had the highest prevalence of HIV in Southeast Asia at 1.1 percent, the 40th highest prevalence of 109 nations.
HIV/AIDS in Bolivia has a less than 1 percent prevalence of Bolivia's adult population estimated to be HIV-positive. Bolivia has one of the lowest HIV prevalence rates in the Latin America and Caribbean region.
Cases of HIV/AIDS in Peru are considered to have reached the level of a concentrated epidemic.
The Dominican Republic has a 0.7 percent prevalence rate of HIV/AIDS, among the lowest percentage-wise in the Caribbean region. However, it has the second most cases in the Caribbean region in total web|url=http://www.avert.org/caribbean-hiv-aids-statistics.htm |title=Caribbean HIV & AIDS Statistics|date=21 July 2015}}</ref> with an estimated 46,000 HIV/AIDS-positive Dominicans as of 2013.
HIV/AIDS in Jamaica has a 1.5 percent prevalence of the adult population estimated to be HIV-positive. There has been no significant change over the last five years and therefore Jamaica appears to have stabilized its HIV/AIDS epidemic.
In 2016, the prevalence rate of HIV/AIDS in adults aged 15–49 was 0.3%, relatively low for a developing country. This low prevalence has been maintained, as in 2006, the HIV prevalence in Mexico was estimated at around 0.3% as well. The infected population is remains mainly concentrated among high risk populations, men who have sex with other men, intravenous drug users, and commercial sex workers. This low national prevalence is not reflected in the high-risk populations. The prison population in Mexico, faces a fairly similar low rate of around 0.7%. Among the population of prisoners, around 2% are known to be infected with HIV. Sex workers, male and female, face an HIV prevalence of around 7%. Identifying gay men and men who have sex with other men have a prevalence of 17.4%. The highest risk-factor group is identifying transgender people; about 17.4% of this population is known to be infected with HIV. Around 90% of new infections occur by sex-related methods of transmission. Of these known infected populations, around 60% of living infected people are known to be on anti-retroviral therapy (ART).
Nicaragua has 0.2 percent of the adult population estimated to be HIV-positive. Nicaragua has one of the lowest HIV prevalence rates in Central America.
With less than 1 percent of the population estimated to be HIV-positive, Egypt is a low-HIV-prevalence country. However, between the years 2006 and 2011, HIV prevalence rates in Egypt increased tenfold. Until 2011, the average number of new cases of HIV in Egypt was 400 per year, but in 2012 and 2013, it increased to about 600 new cases, and in 2014, it reached 880 new cases per year. According to 2016 statistics from UNAIDS, there are about 11,000 people currently living with HIV in Egypt. The Ministry of Health and Population reported in 2020 over 13,000 Egyptians are living with HIV/AIDS. However, unsafe behaviors among most-at-risk populations and limited condom usage among the general population place Egypt at risk of a broader epidemic.
With 1.28 percent of the adult population estimated by UNAIDS to be HIV-positive in 2006, Papua New Guinea has one of the most serious HIV/AIDS epidemics in the Asia-Pacific subregion. Although this new prevalence rate is significantly lower than the 2005 UNAIDS estimate of 1.8 percent, it is considered to reflect improvements in surveillance rather than a shrinking epidemic. Papua New Guinea accounts for 70 percent of the subregion's HIV cases and is the fourth country after Thailand, Cambodia, and Burma to be classified as having a generalized HIV epidemic.
↑ Kharsany, A. B. M.; Kaupilla, D. T. (2021). "Epidemiology of HIV in Sub-Saharan Africa". Nature Reviews Microbiology. 19: 300–313. doi:10.1038/s41579-021-00514-1 (inactive 25 December 2024).{{cite journal}}: CS1 maint: DOI inactive as of December 2024 (link)
↑ Mitchell C, Reid-Walsh J, Pithouse K (2004). "'And what are you reading, Miss? Oh, it is only a website': The New Media and the Pedagogical Possibilities of Digital Culture as a South African 'Teen Guide' to HIV/AIDS and STDs". Convergence: The International Journal of Research into New Media Technologies. 10 (1): 84. doi:10.1177/135485650401000106. S2CID144464356.
1 2 Adebisi, Yusuff Adebayo; Nwogu, Ifechukwu Benedict; Alaran, Aishat Jumoke; Badmos, Abubakar Olaitan; Bamgboye, Adeboye Olakunle; Rufai, Basirat Oluwadamilola; Okonji, Osaretin Christabel; Malik, Malik O.; Teibo, John Oluwafemi; Abdalla, Samah Faisal; Lucero-Prisno, Don Eliseo; Samai, Mohamed; Akande-Sholabi, Wuraola (June 2022). "Revisiting the issue of access to medicines in Africa: Challenges and recommendations". Public Health Challenges. 1 (2). doi:10.1002/puh2.9. ISSN2769-2450.
↑ Feldman-Savelsberg P, Ndonko FT, Schmidt-Ehry B (June 2000). "Sterilizing vaccines or the politics of the womb: retrospective study of a rumor in Cameroon". Medical Anthropology Quarterly. 14 (2): 159–79. doi:10.1525/maq.2000.14.2.159. PMID10879368.
↑ Clements CJ, Greenough P, Shull D (January 2006). "How vaccine safety can become political--the example of polio in Nigeria". Current Drug Safety. 1 (1): 117–9. doi:10.2174/157488606775252575. PMID18690921.
1 2 3 4 Meier, Benjamin Mason: International Protection of Persons Undergoing Medical Experimentation: Protecting the Right of Informed Consent, Berkeley journal of international law [1085-5718] Meier yr:2002 vol:20 iss:3 pg:513 -554
↑ Kunutsor S, Walley J, Muchuro S, Katabira E, Balidawa H, Namagala E, Ikoona E (24 May 2012). "Improving adherence to antiretroviral therapy in sub-Saharan African HIV-positive populations: an enhanced adherence package". AIDS Care. 24 (10): 1308–15. doi:10.1080/09540121.2012.661833. PMID22621288. S2CID13607386.
1 2 Boston, 677 Huntington Avenue; Ma 02115 +1495-1000 (29 June 2018). "The Senegal Sex Workers Study". Harvard AIDS Initiative. Retrieved 18 June 2020.{{cite web}}: CS1 maint: numeric names: authors list (link)
↑ Abdulsalami Nasidi; Tekena O. Harry (2006). "The Epidemiology of HIV/AIDS in Nigeria"(PDF). In Olusoji Adeyi; Phyllis J. Kanki; Oluwole Odutolu (eds.). AIDS in Nigeria: A Nation on the Threshold. Harvard Center for Population and Development Studies: Harvard University Press. pp.17–36. Archived from the original(PDF) on 4 August 2007.
↑ The Political Economy of AIDS in Africa, edited by Nana K. Poku and Alan W. Whiteside, Ashgate Publishing, Ltd., 2004, page 235
↑ Ragnarsson A, Townsend L, Thorson A, Chopra M, Ekstrom AM (October 2009). "Social networks and concurrent sexual relationships--a qualitative study among men in an urban South African community". AIDS Care. 21 (10): 1253–8. doi:10.1080/09540120902814361. PMID20024701. S2CID21008915.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.