

A cluster of patients with an acute severe lower respiratory tract illness linked to a seafood and live animal market was reported by public health officials in Wuhan, Hubei Province, China, in December 2019 (1). Shortly thereafter, the Chinese Center for Disease Control and Prevention commenced an investigation into the outbreak. A previously unknown coronavirus (2019 novel coronavirus [2019-nCoV]) was isolated from respiratory epithelial cells in these patients (2). Initially confined to Wuhan, the infection has spread elsewhere, with 9720 confirmed cases in China and 106 confirmed cases in other countries—including six in the United States as of January 31, 2020 (3,4).
Seven coronaviruses are known to cause disease in humans (2,5,6). Two strains, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV), have zoonotic origins and have been linked to outbreaks of severe respiratory illnesses in humans (6). Although 2019-nCoV, too, is believed to have a zoonotic origin, person-to-person transmission has been documented (7).
Most patients with 2019-nCoV infection present with fever (98%), cough (76%), and myalgia or fatigue (44%). Dyspnea has been reported in 55% of patients, developing in a median of 8 days after onset of initial symptoms. Six of 41 patients (15%) in the largest published cohort to date (8) died from their illness, and there are now 80 confirmed deaths (4).
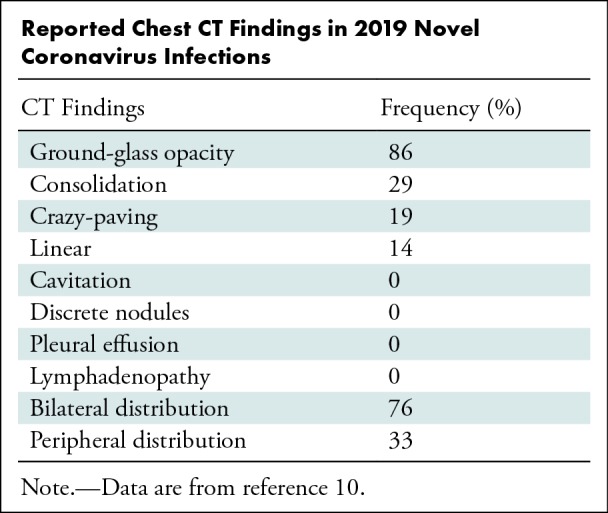
Limited information exists regarding chest imaging findings of 2019-nCoV lung infection (Table). One initial report included chest radiographs of a single patient. A bedside chest radiograph obtained 8 days after symptom onset showed bilateral lung consolidation with relative peripheral sparing. A radiograph obtained 3 days later showed more extensive, basal predominant lung consolidation with possible small pleural effusions corresponding to clinical worsening (2). A second report showed CT images from a single patient who had peripheral, bilateral ground-glass opacity (9). A different report of six family members with 2019-nCoV lung infection mentions lung opacities present on chest CT scans but lacks details on pattern or distribution aside from ground-glass opacities in an asymptomatic 10-year-old boy (7). A recent cohort study of 41 patients with confirmed 2019-nCoV infection included limited analysis of chest imaging studies. All but one patient was reported to have bilateral lung involvement on chest radiographs (8). Patients admitted to the intensive care unit were more likely to have larger areas of bilateral consolidation on CT scans, whereas patients not requiring admission to the intensive care unit with milder illness were more likely to have ground-glass opacity and small areas of consolidation, the latter description suggesting an organizing pneumonia pattern of lung injury. A study of CT scans of 21 patients with 2019-nCoV infection (10) showed three (21%) with normal CT scans, 12 (57%) with ground-glass opacity only, and six (29%) with ground-glass opacity and consolidation at presentation. Fifteen patients (71%) had two or more lobes involved, and 16 (76%) had bilateral disease. Interestingly, three patients (14%) had normal scans at diagnosis. One of those patients still had a normal scan at short-term follow-up. Seven other patients underwent follow-up CT (range, 1–4 days; mean, 2.5 days); five (63%) had mild progression, and two (25%) had moderate progression.
Reported Chest CT Findings in 2019 Novel Coronavirus Infections
Overall, the imaging findings reported for 2019-nCoV are similar to those reported for SARS-CoV (11–13) and MERS-CoV (14,15), not surprising as the responsible viruses are also coronaviruses. Given that up to 30% of patients with 2019-nCoV infection develop acute respiratory distress syndrome (8), chest imaging studies showing extensive consolidation and ground-glass opacity, typical of acute lung injury, are not unexpected (16,17). The long-term imaging features of 2019-nCoV are not yet known but presumably will resemble those of other causes of acute lung injury.
As the number of reported cases of 2019-nCoV infection continue to increase, radiologists may encounter patients with this infection. A high index of suspicion and detailed exposure and travel history are critical to considering this diagnosis. In the correct clinical setting, bilateral ground-glass opacities or consolidation at chest imaging should prompt the radiologist to suggest 2019-nCoV as a possible diagnosis. Furthermore, a normal chest CT scan does not exclude the diagnosis of 2019-nCoV infection.
Footnotes
Disclosures of Conflicts of Interest: Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: is a paid consultant for Parexel International; receives payment for development of educational presentations from Potomoc Continuing Medical Education. Other relationships: disclosed no relevant relationships.
References
- 1.Report of clustering pneumonia of unknown etiology in Wuhan City. Wuhan, China: Wuhan Municipal Health Commission, 2019. [Google Scholar]
- 2.Zhu N, Zhang D, Wang W, et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med doi: 10.1056/NEJMoa2001017. Published online January 25, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.2019 Novel Coronavirus (2019-nCoV) in the U.S . Centers for Disease Control and Prevention https://www.cdc.gov/coronavirus/2019-ncov/cases-in-us.html. Updated February 3, 2020.
- 4.Novel Coronavirus (2019-nCoV) Situation Report 7 . Geneva, Switzerland: World Health Organization. Published online January 27, 2020.
- 5.Su S, Wong G, Shi W, et al. Epidemiology, Genetic Recombination, and Pathogenesis of Coronaviruses. Trends Microbiol 2016;24(6):490–502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cui J, Li F, Shi ZL. Origin and evolution of pathogenic coronaviruses. Nat Rev Microbiol 2019;17(3):181–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chan JF, Yuan S, Kok KH, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet doi: 10.1016/s0140-6736(20)30154-9. Published online January 28, 2020. [DOI] [PMC free article] [PubMed]
- 8.Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet doi: 10.1016/s0140-6736(20)30183-5. Published online January 28, 2020. [DOI] [PMC free article] [PubMed]
- 9.Lei J, Li J, Xiaolong Q. CT Imaging of the 2019 Novel Coronavirus (2019-nCoV) Pneumonia. 10.1148/radiol.2020200236. Published online January 31, 2020. [DOI] [PMC free article] [PubMed]
- 10.Chung M, Bernheim A, Mei X, et al. CT imaging features of 2019 novel coronavirus (2019-nCoV). Radiology (in press). [DOI] [PMC free article] [PubMed]
- 11.Muller NL, Ooi GC, Khong PL, Zhou LJ, Tsang KW, Nicolaou S. High-resolution CT findings of severe acute respiratory syndrome at presentation and after admission. AJR Am J Roentgenol 2004;182(1):39–44. [DOI] [PubMed] [Google Scholar]
- 12.Nicolaou S, Al-Nakshabandi NA, Muller NL. SARS: imaging of severe acute respiratory syndrome. AJR Am J Roentgenol 2003;180(5):1247–1249. [DOI] [PubMed] [Google Scholar]
- 13.Ooi GC, Khong PL, Muller NL, et al. Severe acute respiratory syndrome: temporal lung changes at thin-section CT in 30 patients. Radiology 2004;230(3):836–844. [DOI] [PubMed] [Google Scholar]
- 14.Das KM, Lee EY, Al Jawder SE, et al. Acute Middle East Respiratory Syndrome Coronavirus: Temporal Lung Changes Observed on the Chest Radiographs of 55 Patients. AJR Am J Roentgenol 2015;205(3):W267–274. [DOI] [PubMed] [Google Scholar]
- 15.Das KM, Lee EY, Enani MA, et al. CT correlation with outcomes in 15 patients with acute Middle East respiratory syndrome coronavirus. AJR Am J Roentgenol 2015;204(4):736–742. [DOI] [PubMed] [Google Scholar]
- 16.Desai SR, Wells AU, Rubens MB, Evans TW, Hansell DM. Acute respiratory distress syndrome: CT abnormalities at long-term follow-up. Radiology 1999;210(1):29–35. [DOI] [PubMed] [Google Scholar]
- 17.Desai SR. Acute respiratory distress syndrome: imaging of the injured lung. Clin Radiol 2002;57(1):8–17. [DOI] [PubMed] [Google Scholar]