

Abstract
PURPOSE
The aim of the current study was to report the efficacy of topical and systemic treatments for immune-related cutaneous adverse events (ircAEs) attributed to checkpoint inhibitors in an uncontrolled cohort of patients referred to oncodermatology clinics.
METHODS
A retrospective analysis of patients with ircAEs evaluated by dermatologists from January 1, 2014, to December 31, 2017, at three tertiary care hospitals and cancer centers were identified through electronic medical records. Clinicopathologic characteristics, dermatologic therapy outcome, and laboratory data were analyzed.
RESULTS
A total of 285 patients (median age, 65 years [range, 17 to 89 years]) with 427 ircAEs were included: pruritus (n = 138; 32%), maculopapular rash (n = 120; 28%), psoriasiform rash (n = 22; 5%), and others (n = 147; 34%). Immune checkpoint inhibitor class was associated with ircAE phenotype (P = .007), where maculopapular rash was predominant in patients who received combination therapy. Severity of ircAEs was significantly reduced (mean Common Terminology Criteria for Adverse Events grade: 1.74 v 0.71; P < .001) with dermatologic interventions, including topical corticosteroids, oral antipruritics, and systemic immunomodulators. A total of 88 ircAEs (20%) were managed with systemic immunomodulators. Of these, 22 (25%) of 88 persisted or worsened. In seven patients with corticosteroid-refractory ircAEs, improvement resulted from targeted biologic immunomodulatory therapies that included rituximab and dupilumab. Serum interleukin-6 (IL-6) was elevated in 34 (52%) of 65 patients; grade 3 or greater ircAEs were associated with increased absolute eosinophils (odds ratio, 4.1; 95% CI, 1.3 to 13.4) and IL-10 (odds ratio, 23.8; 95% CI, 2.1 to 262.5); mean immunoglobulin E serum levels were greater in higher-grade ircAEs: 1,093 kU/L (grade 3), 245 kU/L (grade 2), and 112 kU/L (grade 1; P = .043).
CONCLUSION
Most ircAEs responded to symptom- and phenotype-directed dermatologic therapies, whereas biologic therapies were effective in patients with corticosteroid-refractory disease. Increased eosinophils, IL-6, IL-10, and immunoglobulin E were associated with ircAEs, and they may represent actionable therapeutic targets for immune-related skin toxicities.
INTRODUCTION
The emergence of immune checkpoint inhibitors (ICIs) that target the cytotoxic T-lymphocyte-associated antigen-4 (CTLA-4) and programmed death-1/ligand 1 (PD-1/PD-L1) pathways has significantly improved outcomes for patients with a variety of malignancies. Immune-related adverse events (irAEs) attributable to ICI therapy are frequent and may result in treatment interruptions or discontinuation, decreases in quality of life (QoL), morbidity, or even mortality.1-4
Whereas irAEs may affect all organ systems,5 immune-related cutaneous adverse events (ircAEs) are among the most common and earliest to develop, with an incidence of all-grade ircAEs in up to 72% with anti–CTLA-4/anti–PD-1 combination therapy.6 Severity of ircAEs ranges from grade 1 pruritus or maculopapular rash (MPR) to grade 4 Stevens-Johnson syndrome, and severe (grade ≥ 3) ircAEs occur in approximately 2% to 10% of treated patients. Increasing evidence supports the notion that ircAEs, in particular rash and vitiligo among patients with melanoma, are associated with a prolonged progression-free survival and overall survival (OS), which underscores the need for effective supportive care interventions that would permit the maintenance of QoL and dose intensity of ICI.7,8
To date, several irAE management guidelines have been developed, primarily on the basis of case reports, series, experience extrapolated from other autoimmune diseases, and expert consensus. However, the efficacy of various dermatologic treatments included in these guidelines for the management of ircAEs has not been reported. Here, we characterized the clinicopathologic features and management outcomes of ircAEs in a cohort of 285 patients. We also examined laboratory data for potential biomarkers and therapeutic targets that have a putative relation to ircAEs.
PATIENTS AND METHODS
Patients
Patients with a variety of solid tumors treated with anti–CTLA-4 (ipilimumab, tremelimumab), anti–PD-1 (nivolumab, pembrolizumab), or anti–PD-L1 (atezolizumab, avelumab, durvalumab) therapy and referred to the oncodermatology services of Memorial Sloan Kettering Cancer Center (MSK; New York, NY), Columbia University Medical Center (New York, NY), and University Federico II (Naples, Italy) between January 1, 2014, and December 31, 2017, were identified retrospectively using an institutional data management system and a medical imaging software archive (Vectra, Canfield Scientific, Fairfield, NJ). Electronic medical records were reviewed to capture patients who were diagnosed with an ircAE, received dermatologic management, and had follow-up records for assessment of treatment outcomes. A comparator cohort was gathered of ICI recipients at MSK not referred to dermatologists (Data Supplement). This study was conducted under institutional review board–approved protocols for each participating institution.
Assessment and Management of ircAEs
Relevant clinicopathologic data were extracted and analyzed from each patient’s electronic medical record. Diagnosis and grading of ircAEs was done by dermatologists during consultation (A.M. and M.E.L. [MSK]; L.G. [Columbia University Medical Center]; and G.F. [University Federico II]), oncology physicians, or advanced practice providers. ircAEs were graded using the Common Terminology Criteria for Adverse Events, version 4.0.9
Clinical treatment responses were arbitrarily classified as significant improvement (improvement by two or more grades or an improvement to grade 0), moderate improvement (a one-grade improvement), or no improvement (no change or increase in grade). Corticosteroid-refractory ircAEs were defined as those in which there was no response or in which ircAE worsening occurred during or after one or more courses of systemic corticosteroids at prednisone 0.5 to 1 mg/kg per day or equivalent.
Laboratory data obtained within 1 month of dermatology visits was included for analysis: hemogram, basic or comprehensive metabolic panels, and serum levels of interleukin (IL)-1β, IL-5, IL-6, IL-8, IL-10, interferon-gamma (IFNγ), tumor necrosis factor-α (TNF-α), immunoglobulin E (IgE), elafin, histamine, and tryptase.
Statistical Methods
Data were summarized using descriptive statistics. Comparisons of categorical variables were performed using the χ2 test and those of continuous or ordinal variables by analysis of variance, Mann-Whitney U, or Kruskal-Wallis tests. OS analysis was conducted using Kaplan-Meier and log-rank analyses. All statistical tests were two sided and considered statistically significant if P < .05. Statistical analyses were performed using Excel (Microsoft, Redmond, WA) and SPSS Statistics version 24 (IBM, Armonk, NY).
RESULTS
Patient Demographics
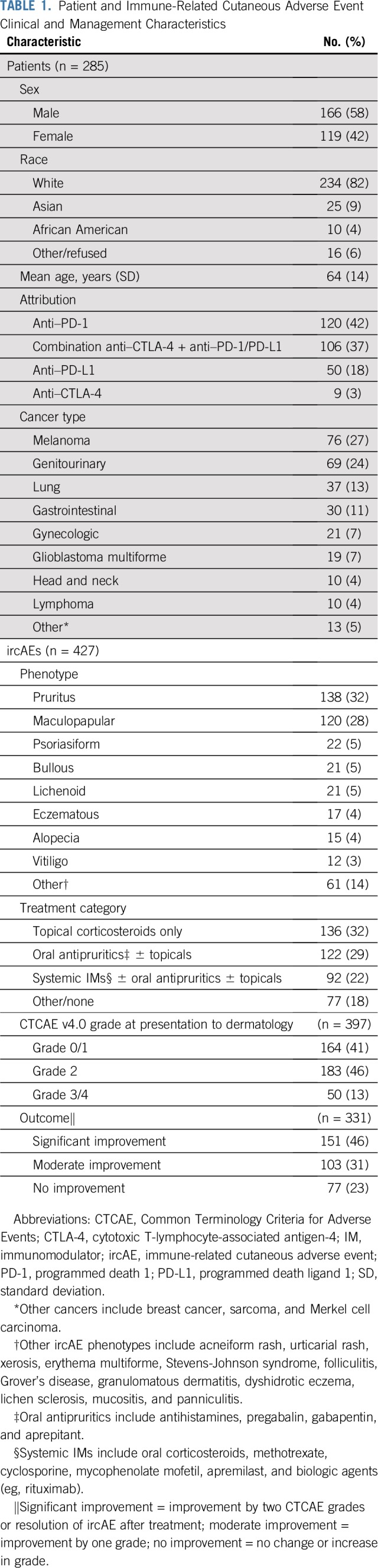
A total of 285 patients referred by 100 oncologists were included in the analysis, with a median age of 65 years (range, 17 to 89 years; Table 1). Referral patterns across the three participating centers mirrored ICI use at MSK, with the majority of referrals being requested by solid tumor oncologists (Data Supplement). Duration of treatment ranged from 1 day to 2,277 days with a median of 224 days (interquartile range [IQR], 84 to 459 days).
TABLE 1.
Patient and Immune-Related Cutaneous Adverse Event Clinical and Management Characteristics
ircAE Characteristics and Clinical Course
Of 285 patients with ircAEs, 131 patients (46%) developed one or more events for a total of 427 ircAEs (Table 1). The most common ircAEs were pruritus (n = 138; 32%) and MPR (n = 120; 28%; Fig 1). Although no association was found between primary cancer diagnosis and ircAE phenotype (P = .19), 11 (92%) of 12 vitiligo-like depigmentation events occurred in patients with melanoma; one event developed in a patient with renal cell carcinoma after 21 cycles of atezolizumab plus bevacizumab. There was an association between ICI class and ircAE phenotype, such that bullous pemphigoid-like eruptions constituted 7% of ircAEs that were attributed to anti–PD-1/PD-L1 monotherapy versus 2% of ircAEs that were attributed to anti–CTLA-4 with or without anti–PD-1/PD-L1 agents (P = .003). Conversely, targeting CTLA-4 with or without anti-PD-1/PD-L1 therapy was associated with MPR (36% of ircAEs attributed to anti-CTLA-4 with or without anti-PD-1/PD-L1 were MPR compared with 23% of ircAEs that were attributed to anti–PD-1/PD-L1 monotherapy; P = .008; Fig 2).
FIG 1.

Clinical manifestation of immune-related cutaneous adverse events before (left) and after (right) treatment. (A) Patient with melanoma receiving ipilimumab plus nivolumab with grade 3 maculopapular rash managed with oral prednisone. (B) Patient with lymphoma receiving chemotherapy plus atezolizumab with grade 2 psoriasiform rash treated with ustekinumab. (C) Patient with melanoma receiving nivolumab with grade 3 bullous pemphigoid-like eruption treated with rituximab. (D) Patient with renal-cell carcinoma on nivolumab with grade 3 eczematous rash and pruritus managed with dupilumab.
FIG 2.

Immune checkpoint inhibitor (ICI) type and associated immune-related cutaneous adverse event (ircAE) phenotypes. Bar height represents the proportion of ircAEs of specified phenotype attributable to either anti–cytotoxic T-lymphocyte-associated antigen-4 (CTLA-4) with or without anti–programmed death 1 (PD-1)/programmed death ligand 1 (PD-L1) or anti–PD-1/PD-L1 monotherapy. Values within columns reflect the absolute frequency of ircAE attributable to ICI therapy. MPR, maculopapular rash.
Most ircAEs were grade 1 to 2 in severity (n = 347; 87%). Grade 3 to 4 ircAEs included 24 events of MPR (48%), six pruritus (12%), four bullous pemphigoid-like eruption (8%), four Stevens-Johnson syndrome (8%), three lichenoid rash (6%), two psoriasiform rash (4%), and seven others (14%). No grade 5 ircAEs were observed. There was no association between ircAE severity and ICI type (P = .37). Severity of ircAEs was greater in patients who were referred to dermatology compared with those treated by oncologists for ircAEs (63% v 19% grade ≥ 2; P < .001; Data Supplement).
Median time from the initiation of treatment to presentation to the dermatologist was 119 days (IQR, 40 to 322 days; range, 1 to 2,380 days). MPR presented earlier than other ircAEs (62 days v 133 days; P < .001). For grade 3 to 4 ircAEs, median time to presentation was 77.5 days (IQR, 13.5 to 343 days; Fig 3). OS, defined as ICI initiation to death from any cause, was longer for patients who were evaluated by dermatologists than for nondermatology-evaluated patients (median survival time 62 months [95% CI, 36 to 88 months] v 20 months [95% CI, 18 to 22 months]; P < .001; Data Supplement).
FIG 3.

Time to presentation to dermatology and resolution of immune-related cutaneous adverse events (ircAEs). Boxes represent interquartile range (IQR; Q1, Q3), central vertical line indicates median, outer vertical lines indicate range or Q3 + (1.5 × IQR) for subsets with outliers, and text indicates range inclusive of outliers (minimum to maximum [min-max]). (A) For time to presentation, number indicates ircAE frequency. (B) For time to resolution, number indicates ircAEs that resolved. IM, systemic immunomodulator; min-max, minimum-maximum; MPR, maculopapular rash.
Management and Treatment Outcomes of ircAEs
Common treatment strategies included topical corticosteroids, systemic antipruritics (eg, gabapentin/pregabalin, aprepitant, and antihistamines), and systemic immunomodulators (IMs; eg, oral corticosteroids, antimetabolite agents, calcineurin inhibitors, and monoclonal antibodies that target immune pathways), singly and in combination. Topical agents were prescribed to 213 patients (75%), of which 94 (44%) received topical agents alone. One hundred thirty-three patients (47%) were prescribed systemic therapies for their ircAEs (Table 1). Treatment patterns did not differ between dermatologists (P = .06). Of 58 patients (20%) who were treated with IMs, 51 (88%) received oral corticosteroids. Patients with psoriasiform and bullous ircAEs more frequently required the use of IMs compared with patients with other ircAEs (patients with psoriasiform, 61%; patients with bullous, 39%; all patients, 20%; P < .001). Patients who were treated with IMs had higher-grade ircAEs compared with patients who were treated with topical therapies (mean grade, 2.23 v 1.53; P < .001).
Of those ircAEs with both initial and follow-up grades recorded (n = 331), there was a significant difference between grade at diagnosis and follow-up (mean grade, 1.74 v 0.71; P < .001; mean grade reduction, −1.04; standard deviation, 0.90). The largest improvement was observed in MPR (mean grade reduction, −1.40; standard deviation, 0.96). Forty of 44 grade 3 to 4 ircAEs improved with therapy (91% v 75% grade ≤ 2; P = .02), most frequently as a result of IMs (22 [55%] of 40 responding AEs). Twenty-two (25%) of 88 ircAEs were refractory to IMs, of which 19 (86%) were corticosteroid refractory. Figure 4 details the frequency of ircAE response to treatment stratified by ircAE phenotype (MPR, pruritus, psoriasiform rash, etc) and treatment category (topical corticosteroids alone, oral antipruritics with or without topical corticosteroids, IMs with or without topical corticosteroids or oral antipruritics, and other or supportive treatments not captured above). In ircAEs overall, topical corticosteroids and oral antipruritics resulted in more frequent significant improvement compared with IMs (topicals, 56%; antipruritics, 48%; IMs, 26%; P < .001). In addition, in those adverse events treated with topical agents alone (n = 119; 37%), the superpotent topical corticosteroid clobetasol—74 (66%) of 119—was not superior to less potent topical corticosteroids (P = .07). Treatment outcome was higher at MSK compared with other sites (79% v 62% response; P = .03), and there was no difference in outcome between providers at MSK (P = .4).
FIG 4.

Immune-related cutaneous adverse event (ircAE) management and outcomes. Bars depict the frequency of ircAEs managed within a particular treatment category, and bar color corresponds to outcome category (no improvement, moderate improvement, significant improvement). Percentages after bars reflect ircAE response rate to therapy—rate of moderate or significant improvement—within the particular treatment category. Significant improvement = improvement by 2 Common Terminology Criteria for Adverse Events grades or resolution of ircAE; moderate improvement = improvement by 1 grade; no improvement = no change or increase in grade. Other ircAE phenotypes include eczematous rash, acneiform rash, urticarial rash, vitiligo, alopecia, xerosis, erythema multiforme, Stevens-Johnson syndrome, folliculitis, Grover disease, granulomatous dermatitis, dyshidrotic eczema, lichen sclerosis, mucositis, and panniculitis. Topicals refers to topical corticosteroid use alone. Oral antipruritics include antihistamines, pregabalin, gabapentin, and aprepitant with and without the use of topical corticosteroids. Systemic immunomodulators (IMs) include oral corticosteroids, methotrexate, cyclosporine, mycophenolate mofetil, apremilast, and biologic agents (eg, rituximab) with and without the use of topical corticosteroids or oral antipruritics. (*) Outcome distribution significantly associated with ircAE treatment category (Pearson χ2, overall, P < .001; pruritus, P = .03; lichenoid, P = .02). MPR, maculopapular rash.
Pruritus was most frequently managed with oral antipruritics with or without the addition of topical corticosteroids and without the need for IMs (n = 55; 40%), most of which demonstrated a moderate to significant improvement after treatment (39 [87%] of 45). GABA (γ-aminobutyric acid) analogs pregabalin and gabapentin resulted in moderate to significant improvement in 17 (100%) of 17 patients, whereas oral antihistamines showed benefit in 13 (81%) of 16 patients.
Biologic monoclonal antibody therapy was used to treat corticosteroid-refractory or dependent ircAEs in seven patients as a rational approach in accordance to putative mechanisms of toxicity (Data Supplement). Three patients received rituximab for bullous pemphigoid-like eruption, two received dupilumab—anti–IL-4 receptor α—for eczematous rash, and guselkumab—anti–IL-23 α subunit—and ustekinumab—anti–IL-12/IL-23—were administered in one patient each for psoriasiform rash. These patients experienced a moderate to significant improvement in their corticosteroid-refractory ircAEs (n = 7; 100%). Of three patients who were treated with biologic agents who achieved tumor response, it was maintained. Two other patients experienced progression of their cancer before biologic therapy, and in the other two patients, no follow-up imaging was available to ascertain response.
Histopathology and Laboratory Findings of ircAEs
We analyzed the histopathologic samples of ircAEs from 70 skin biopsies obtained from 65 patients (Data Supplement). We identified a spectrum of pathologic findings in ircAEs, unified by a perivascular (51%) and/or interface (50%) dermatitis that consisted of a lymphocytic inflammatory infiltrate (57%; six of six with immunostaining showed CD3+ T-cell predominance and three of these quantified CD4:CD8 ratios: alopecia, 2:1; MPR, 3:1; eczematous rash, 5:1), accompanied by eosinophils in 51% and occasionally spongiosis (29%) in the epidermis, all reported with drug hypersensitivity reactions. There was no statistically significant association between the presence of histologic features and ircAE severity or outcome (P > .08).
The most commonly elevated serum analytes were IL-6 (34 [52%] of 65), elafin (13 [30%] of 43), IL-8 (five [25%] of 20), IgE (24 [24%] of 101), and IFNγ (six [23%] of 26) (Data Supplement). Seventeen eosinophil-related ircAEs were recorded in 13 (5%) of 273 patients, which were characterized by rash and pruritus. Correspondingly, eosinophilia was associated with grade 3 or greater ircAEs (odds ratio, 4.1; 95% CI, 1.3 to 13.4). Patients with grade 3 or greater ircAEs had elevated serum IL-10 (five [56%] of nine) more frequently than did those with grade 2 or less events (one [5%] of 20; P = .005; odds ratio, 23.8; 95% CI, 2.1 to 262.5). Furthermore, IgE serum level correlated with ircAE severity (mean IgE, 112 kU/L [grade 1] v 245 kU/L [grade 2] v 1,093 kU/L [grade 3]; P = .043).
DISCUSSION
As ircAEs represent a significant toxicity burden,2-4,10-12 we sought to characterize these untoward reactions and their dermatologic management in order to propose a practical treatment algorithm with the potential to improve QoL and optimize clinical outcomes.
Characterization of ircAEs
The majority of patients in our dermatology-evaluated cohort presented with MPR (42%) or pruritus (48%), which is consistent with their reported incidence in controlled trials. A subset of patients developed psoriasiform (7%) or lichenoid rash (7%) and bullous pemphigoid-like eruption (7%).6,13-28 Vitiligo-like depigmentation was identified in one patient with metastatic renal cell carcinoma treated with atezolizumab plus bevacizumab. Indeed, vitiligo-like depigmentation has been reported in 2.0% to 8.3% of patients with melanoma treated with ICIs17,29 and has only been reported anecdotally in 14 patients with other malignancies.20,30-40 In addition, mono- or combination therapy that involved anti–CTLA-4 agents preferentially resulted in MPR, whereas anti–PD-1/PD-L1 monotherapies resulted in more lichenoid, psoriasiform, and bullous reactions, as previously described.41 Combination therapy has been associated with increased frequency, severity, and acuity of ircAEs; however, this was not observed in our cohort, likely as a result of a bias toward referral of high-grade ircAEs. Moreover, patients with combination therapy–induced ircAEs are usually treated with high-dose corticosteroids in a first-line setting by the primary oncologist.6,12,17,42
Median time to presentation of all-grade ircAEs was longer than that of grade 3 to 4 ircAE, which is reflective of a lower severity grade being less urgent.43 Median time to ircAE resolution was 44 days, which is lower than that reported with combination ICIs (79 days) or with single-agent nivolumab (126 days).43,44 These differences may reflect the efficacy of ircAE management by oncodermatologists or may also have resulted from a lead-time bias.
ircAE severity and OS were greater in patients who were evaluated by dermatology compared with those who were not. Taken together, these results corroborate previous research that correlates the presence of ircAEs with improved survival, and they might suggest that the presence of more severe ircAEs that warrant referral to dermatology parallels a more robust antitumor response.7,8,44-46 However, greater OS in the study cohort may be explained in part by ICI treatment duration, whereby longer treatment leads to both prolonged survival and more time for ircAEs to develop. In addition, patient functional status might confound survival as patients generally need better functional status or support systems to attend multiple outpatient dermatology appointments.
ircAE Pathomechanism and Associated Biomarkers
Few candidate biomarkers related to organ-specific irAEs have been reported.47-49 In the skin, molecular profiling of affected cutaneous tissues has suggested that specific chemokines and cytokines are etiopathogenic, including PI3, SPRR2B, GZMB, CXCL9, CXCL10, and CXCL11.28,50-53 Histologic findings in our study were consistent with previous reports,54-58 showing a mixed inflammatory infiltrate with a predominance of T cells, neutrophils, or eosinophils, with features of hypersensitivity, which underscores the presence of cells that may represent therapeutic targets.
Circulating proinflammatory cytokines, including IL-1α, IL-1β, IL-2, and IFNα2, have been correlated with grade 3 or greater irAEs in patients with melanoma receiving anti–PD-1 therapy.59 We identified correlations between increased laboratory analytes (eosinophil counts; IL-6, IL-10, and IgE levels) and grade 3 or greater ircAEs, which suggest pathogenic or correlative roles and potential targets for supportive care interventions. Indeed, anti–IL-6 therapy has been successfully used to treat irAEs60-62 including cytokine release syndrome,63-66 and the anti-IgE antibody omalizumab is approved for the treatment of the pruritic disorder chronic idiopathic urticaria,67 which shares clinical and laboratory features with ICI-related pruritus—that is, resistance to antihistamines or corticosteroids and increased serum IgE levels.68
Treatment Efficacy of ircAEs
Patients reported in the work represent, to our knowledge, the largest cohort to date of ircAE treatment outcomes. The majority of patients achieved one to two grade reductions in severity and/or complete resolution of their ircAEs as a result of supportive topical and/or systemic interventions. Consequently, we have produced a treatment schema that is based on our experience to date and have provided retrospective justification of its potential efficacy (Fig 5). Our proposed treatment algorithm differs from published guidelines in its inclusion of psoriasiform and lichenoid rash and consideration of targeted agents for corticosteroid-refractory ircAEs.
FIG 5.

Proposed algorithm for the management of immune-related cutaneous adverse events. ICI, immune checkpoint inhibitor; IgE, immunoglobulin E; IL-6, interleukin-6; MPR, maculopapular rash; NB-UVB, narrowband UV B; OTC, over the counter.
Pruritus is a common ircAE that has been shown to negatively affect QoL.68 We report efficacy of GABA analogs—gabapentin and pregabalin—and the neurokinin-1 receptor antagonist aprepitant, which seem to be superior to topical corticosteroids and oral antihistamines. These findings are supported by data in other patient populations. Pregabalin has demonstrated robust efficacy against uremic pruritus in controlled studies,69 whereas aprepitant has shown benefit in targeted therapy–induced pruritus refractory to antihistamines and topical corticosteroids.70
MPR proved more readily manageable—often with topical interventions alone—whereas other ircAEs, such as psoriasiform rash, demonstrated less favorable outcomes. Furthermore, there was an apparent difference in outcome between management categories in which ircAEs that were treated with IMs had lower rates of significant improvement compared with ircAEs treated with non-IM agents. This may be confounded by sampling factors that affected treatment allocation, such as ircAE severity and refractoriness to less aggressive therapies, patient functional status and preference, restricted access to biologic therapies, or by analytical factors that included the tendency of the outcome schema to favor significant over moderate improvement among grade 1 ircAEs as a reduction to grade 0 was considered a significant improvement even when it resulted from a one-grade improvement.
Although systemic corticosteroids remain the mainstay of management for most grade 2 or greater irAEs, they are not always effective and may affect the antitumor efficacy of ICIs when used at high doses or at the initiation of ICI therapy.71-73 Recommendations for the management of corticosteroid-refractory irAEs include IMs, such as mycophenolate mofetil, calcineurin inhibitors, methotrexate, tumor necrosis factor inhibitors, intravenous immunoglobulin, and plasmapheresis; however, there is little to no data on their efficacy or safety in ICI-treated patients.5,10-12,15,53,74-79 Hence, we report that agents that blocked CD20, IL-4Rα, IL-23α, and IL-12/IL-23 demonstrated benefit in seven patients with corticosteroid-refractory ircAEs80 (Data Supplement). In these patients, pretreatment tumor responses were maintained despite the administration of these IMs. Given a more targeted inhibition of inflammatory cells and their mediators compared with corticosteroids, these agents have the potential to mitigate irAEs without affecting the antitumor efficacy of ICIs. However, these observations require additional studies to assess IM efficacy and safety.
Limitations
As dermatology consultation was an inclusion criterion for our retrospective analysis of medical records and clinical trial case report forms, the generalizability to grade 1 to 2 ircAEs that do not reach a dermatologist may be limited. Our data did not show an association of ICI type with ircAE grade, possibly as a result of limited sample size or increased grade 2 to 3 ircAEs in our study. In addition, dermatologic management may have been influenced by patient preference and health insurance medication coverage, which reflects the real-world clinical scenario of ircAE management, but also limits which treatments were available for analysis. Furthermore, the outcome of targeted biologic agents for ircAE management and sampling for biomarker analysis is limited by sample size and selection bias, which makes it difficult to draw strong conclusions from these data.
In conclusion, the majority of patients with ircAEs were treated effectively with topical or oral corticosteroids (for rash and pruritus); GABA analogs (for pruritus); antihistamines or neurokinin-1 receptor inhibitors (for pruritus); and CD20, IL-4Rα, IL-23α, and IL-12/IL-23 inhibitors (for corticosteroid-refractory ircAEs). As the use of ICI therapies enters additional tumor types and the adjuvant or neoadjuvant settings, an improved understanding and management of ircAEs is essential. The identification of effective therapies for ircAEs and corticosteroid-refractory ircAEs described herein represents the first step toward the design of controlled trials that would demonstrate their safety and efficacy. These findings would eventually be translated to irAEs that affect other organ systems, all of which would be critical for the optimization of ICI therapies.
ACKNOWLEDGMENT
The authors thank Bernadette Murphy for clinical photography.
Footnotes
Presented at the 2018 American Society of Clinical Oncology Annual Meeting, Chicago, IL, June 1-5, 2018.
Funded in part by National Cancer Institute Cancer Center Support Grants No. P30-CA008748 and R25-CA020449, as well as by Beca Excelencia Fundación Piel Sana (A.F.-M.).
The content is solely the responsibility of the authors and does not necessarily represent the official views of the US National Institutes of Health. The sponsors had no role in the design and conduct of the study; in the collection, analysis, and interpretation of data; in the preparation, review, or approval of the manuscript; or in the decision to submit the manuscript for publication.
See accompanying Oncology Grand Rounds on page 2714
AUTHOR CONTRIBUTIONS
Conception and design: Gregory S. Phillips, Jennifer Wu, Robert J. Motzer, Larisa Geskin, Chih-Hsun Yang, Wen-Hung Chung, Mario E. Lacouture
Administrative support: Gregory S. Phillips, Stephen Dusza, Chih-Hsun Yang, Mario E. Lacouture
Provision of study materials or patients: Matthew D. Hellmann, Michael A. Postow, Robert J. Motzer, Jonathan E. Rosenberg, Margaret K. Callahan, Larisa Geskin, Mario E. Lacouture
Collection and assembly of data: Gregory S. Phillips, Jennifer Wu, Matthew D. Hellmann, Naiyer A. Rizvi, Azael Freites-Martinez, Donald Chan, Robert J. Motzer, Jonathan E. Rosenberg, Margaret K. Callahan, Larisa Geskin, Adriana T. Lopez, Vanessa A. Reed, Gabriella Fabbrocini, Maria Carmela Annunziata, Oluwaseun Kukoyi, Aliyah Pabani, Wen-Hung Chung, Alina Markova, Mario E. Lacouture
Data analysis and interpretation: Gregory S. Phillips, Jennifer Wu, Matthew D. Hellmann, Michael A. Postow, Donald Chan, Stephen Dusza, Robert J. Motzer, Jonathan E. Rosenberg, Margaret K. Callahan, Paul B. Chapman, Larisa Geskin, Wen-Hung Chung, Alina Markova, Mario E. Lacouture
Manuscript writing: All authors
Final approval of manuscript: All authors
Accountable for all aspects of the work: All authors
AUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Treatment Outcomes of Immune-Related Cutaneous Adverse Events
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Matthew D. Hellmann
Stock and Other Ownership Interests: Shattuck Labs
Honoraria: AstraZeneca, Bristol-Myers Squibb
Consulting or Advisory Role: Bristol-Myers Squibb, Merck, Genentech, AstraZeneca, MedImmune, Novartis, Janssen Pharmaceuticals, Nektar, Syndax, Mirati Therapeutics, Shattuck Labs
Research Funding: Bristol-Myers Squibb (Inst)
Patents, Royalties, Other Intellectual Property: A patent has been filed by Memorial Sloan Kettering (PCT/US2015/062208) for the use of tumor mutation burden for prediction of immunotherapy efficacy, licensed to Personal Genome Diagnostics (Inst)
Travel, Accommodations, Expenses: AstraZeneca, Bristol-Myers Squibb
Michael A. Postow
Honoraria: Bristol-Myers Squibb, Merck
Consulting or Advisory Role: Bristol-Myers Squibb, Novartis, Array BioPharma, Newlink Genetics, Incyte, Merck, Aduro Biotech
Research Funding: Bristol-Myers Squibb (Inst), Novartis (Inst), Array BioPharma (Inst), Infinity Pharmaceuticals (Inst), Rgenix (Inst), Merck (Inst), AstraZeneca (Inst), MedImmune (Inst)
Naiyer A. Rizvi
Leadership: ARMO BioSciences
Stock and Other Ownership Interests: Gritstone Oncology, ARMO BioSciences, Bellicum Pharmaceuticals, Brooklyn ImmunoTherapeutics
Consulting or Advisory Role: AstraZeneca, MedImmune, Genentech, Novartis, Merck Sharp & Dohme, Bristol-Myers Squibb, Pfizer, Eli Lilly, AbbVie, Regeneron, Janssen Pharmaceuticals, EMD Serono, GlaxoSmithKline, NeoGenomics Laboratories
Research Funding: Bristol-Myers Squibb, Merck Sharp & Dohme
Patents, Royalties, Other Intellectual Property: Royalties related to patent filed by Memorial Sloan Kettering Cancer Center, determinants of cancer response to immunotherapy (PCT/US2015/062208), licensed to Personal Genome Diagnostics
Azael Freites-Martinez
Travel, Accommodations, Expenses: ISDIN, Cantabria Labs, Mylan, Pierre Fabre
Robert J. Motzer
Consulting or Advisory Role: Pfizer, Novartis, Eisai, Exelixis, Merck, Genentech, Incyte, Eli Lilly
Research Funding: Pfizer (Inst), Bristol-Myers Squibb (Inst), Eisai (Inst), Novartis (Inst), Genentech (Inst)
Jonathan E. Rosenberg
Stock and Other Ownership Interests: Merck, Illumina
Honoraria: UpToDate, Bristol-Myers Squibb, AstraZeneca, Medscape, Vindico, Peerview, Chugai Pharma
Consulting or Advisory Role: Eli Lilly, Merck, Agensys, Genentech, Sanofi, AstraZeneca, MedImmune, Bristol-Myers Squibb, EMD Serono, Seattle Genetics, Bayer, Inovio Pharmaceuticals, BioClin Therapeutics, QED Therapeutics, Adicet Bio, Sensei Biotherapeutics, Fortress Biotech, Pharmacyclics, Western Oncolytics
Research Funding: Genentech (Inst), Oncogenex (Inst), Agensys (Inst), Mirati Therapeutics (Inst), Novartis (Inst), Viralytics (Inst), Genentech (Inst), Incyte (Inst), Seattle Genetics (Inst), Bayer (Inst), AstraZeneca (Inst)
Patents, Royalties, Other Intellectual Property: Predictor of platinum sensitivity (Inst)
Travel, Accommodations, Expenses: Genentech, Bristol-Myers Squibb
Margaret K. Callahan
Employment: Bristol-Myers Squibb (I), Celgene (I), Kleo Pharmaceuticals (I), Bristol-Myers Squibb (I)
Consulting or Advisory Role: AstraZeneca, Moderna Therapeutics, Merck
Research Funding: Bristol-Myers Squibb (Inst)
Other Relationship: Clinical Care Options, Potomac Center for Medical Education
Paul B. Chapman
Stock and Other Ownership Interests: Rgenix
Consulting or Advisory Role: Bristol-Myers Squibb, Genentech, Takeda, Cell Medica, Merck, Immunocore
Research Funding: Pfizer
Larisa Geskin
Honoraria: Mallinckrodt, Helsinn Therapeutics
Consulting or Advisory Role: Medivir, Helsinn Therapeutics, Actelion, Mallinckrodt
Speakers' Bureau: Helsinn Therapeutics
Research Funding: Actelion, Mallinckrodt, Bristol-Myers Squibb
Travel, Accommodations, Expenses: Helsinn Therapeutics
Vanessa A. Reed
Consulting or Advisory Role: AstraZeneca
Travel, Accommodations, Expenses: AstraZeneca
Aliyah Pabani
Consulting or Advisory Role: AstraZeneca
Alina Markova
Honoraria: AstraZeneca
Consulting or Advisory Role: AstraZeneca
Research Funding: Incyte
Mario E. Lacouture
Consulting or Advisory Role: Novocure, Legacy Healthcare Services, Janssen Research & Development, Adgero Biopharmaceuticals, Galderma, Amryt Pharmaceuticals, Lindi, Debiopharm Group, Merck, Legacy Healthcare Services, Helsinn Healthcare, Celldex, Menlo Therapeutics, Johnson & Johnson, Roche, AbbVie, Boehringer Ingelheim, Allergan, Amgen, EE Squibb & Sons, EMD Serono, AstraZeneca, Genentech, LEO Pharma, Seattle Genetics, Bayer, Manner SAS, Lutris, Pierre Fabre, Roche, Paxman Coolers, Adjucare, Dignitana, Biotechspert, Parexel, Novartis, F Hoffmann La Roche, Teva, OnQuality Pharmaceuticals, Our Brain Bank, Millennium Pharmaceuticals
Research Funding: Veloce (Inst), US Biotest (Inst), Berg (Inst), Bristol-Myers Squibb, (Inst) Lutris (Inst), Paxman (Inst), Novocure (Inst)
No other potential conflicts of interest were reported.
REFERENCES
- 1.Malkhasyan KA, Zakharia Y, Milhem M. Quality-of-life outcomes in patients with advanced melanoma: A review of the literature. Pigment Cell Melanoma Res. 2017;30:511–520. doi: 10.1111/pcmr.12647. [DOI] [PubMed] [Google Scholar]
- 2.Wang DY, Salem JE, Cohen JV, et al. Fatal toxic effects associated with immune checkpoint inhibitors: A systematic review and meta-analysis. JAMA Oncol. 2018;4:1721–1728. doi: 10.1001/jamaoncol.2018.3923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shoushtari AN, Friedman CF, Navid-Azarbaijani P, et al. Measuring toxic effects and time to treatment failure for nivolumab plus ipilimumab in melanoma. JAMA Oncol. 2018;4:98–101. doi: 10.1001/jamaoncol.2017.2391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Brahmer JR, Rodríguez-Abreu D, Robinson AG, et al. Health-related quality-of-life results for pembrolizumab versus chemotherapy in advanced, PD-L1-positive NSCLC (KEYNOTE-024): A multicentre, international, randomised, open-label phase 3 trial. Lancet Oncol. 2017;18:1600–1609. doi: 10.1016/S1470-2045(17)30690-3. [DOI] [PubMed] [Google Scholar]
- 5.Puzanov I, Diab A, Abdallah K, et al. Managing toxicities associated with immune checkpoint inhibitors: Consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J Immunother Cancer. 2017;5:95. doi: 10.1186/s40425-017-0300-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sibaud V. Dermatologic reactions to immune checkpoint inhibitors: Skin toxicities and immunotherapy. Am J Clin Dermatol. 2018;19:345–361. doi: 10.1007/s40257-017-0336-3. [DOI] [PubMed] [Google Scholar]
- 7.Sanlorenzo M, Vujic I, Daud A, et al. Pembrolizumab cutaneous adverse events and their association with disease progression. JAMA Dermatol. 2015;151:1206–1212. doi: 10.1001/jamadermatol.2015.1916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Freeman-Keller M, Kim Y, Cronin H, et al. Nivolumab in resected and unresectable metastatic melanoma: Characteristics of immune-related adverse events and association with outcomes. Clin Cancer Res. 2016;22:886–894. doi: 10.1158/1078-0432.CCR-15-1136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) version 4.03. https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_4.03.xlsx
- 10.Naidoo J, Page DB, Li BT, et al. Toxicities of the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies. Ann Oncol. 2015;26:2375–2391. doi: 10.1093/annonc/mdv383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Weber JS, Kähler KC, Hauschild A. Management of immune-related adverse events and kinetics of response with ipilimumab. J Clin Oncol. 2012;30:2691–2697. doi: 10.1200/JCO.2012.41.6750. [DOI] [PubMed] [Google Scholar]
- 12.Weber JS, Dummer R, de Pril V, et al. Patterns of onset and resolution of immune-related adverse events of special interest with ipilimumab: Detailed safety analysis from a phase 3 trial in patients with advanced melanoma. Cancer. 2013;119:1675–1682. doi: 10.1002/cncr.27969. [DOI] [PubMed] [Google Scholar]
- 13.Bonigen J, Raynaud-Donzel C, Hureaux J, et al. Anti-PD1-induced psoriasis: A study of 21 patients. J Eur Acad Dermatol Venereol. 2017;31:e254–e257. doi: 10.1111/jdv.14011. [DOI] [PubMed] [Google Scholar]
- 14.Nayar N, Briscoe K, Fernandez Penas P. Toxic epidermal necrolysis-like reaction with severe satellite cell necrosis associated with nivolumab in a patient with ipilimumab refractory metastatic melanoma. J Immunother. 2016;39:149–152. doi: 10.1097/CJI.0000000000000112. [DOI] [PubMed] [Google Scholar]
- 15.Eigentler TK, Hassel JC, Berking C, et al. Diagnosis, monitoring and management of immune-related adverse drug reactions of anti-PD-1 antibody therapy. Cancer Treat Rev. 2016;45:7–18. doi: 10.1016/j.ctrv.2016.02.003. [DOI] [PubMed] [Google Scholar]
- 16.Michot JM, Bigenwald C, Champiat S, et al. Immune-related adverse events with immune checkpoint blockade: A comprehensive review. Eur J Cancer. 2016;54:139–148. doi: 10.1016/j.ejca.2015.11.016. [DOI] [PubMed] [Google Scholar]
- 17.Belum VR, Benhuri B, Postow MA, et al. Characterisation and management of dermatologic adverse events to agents targeting the PD-1 receptor. Eur J Cancer. 2016;60:12–25. doi: 10.1016/j.ejca.2016.02.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Liu J, Blake SJ, Harjunpää H, et al. Assessing immune-related adverse events of efficacious combination immunotherapies in preclinical models of cancer. Cancer Res. 2016;76:5288–5301. doi: 10.1158/0008-5472.CAN-16-0194. [DOI] [PubMed] [Google Scholar]
- 19.Judd J, Zibelman M, Handorf E, et al. Immune-related adverse events as a biomarker in non-melanoma patients treated with programmed cell death 1 inhibitors. Oncologist. 2017;22:1232–1237. doi: 10.1634/theoncologist.2017-0133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Larsabal M, Marti A, Jacquemin C, et al. Vitiligo-like lesions occurring in patients receiving anti-programmed cell death-1 therapies are clinically and biologically distinct from vitiligo. J Am Acad Dermatol. 2017;76:863–870. doi: 10.1016/j.jaad.2016.10.044. [DOI] [PubMed] [Google Scholar]
- 21.Habre M, Habre SB, Kourie HR. Dermatologic adverse events of checkpoint inhibitors: What an oncologist should know. Immunotherapy. 2016;8:1437–1446. doi: 10.2217/imt-2016-0074. [DOI] [PubMed] [Google Scholar]
- 22.Minkis K, Garden BC, Wu S, et al. The risk of rash associated with ipilimumab in patients with cancer: A systematic review of the literature and meta-analysis. J Am Acad Dermatol. 2013;69:e121–e128. doi: 10.1016/j.jaad.2012.12.963. [DOI] [PubMed] [Google Scholar]
- 23.Sibaud V, Meyer N, Lamant L, et al. Dermatologic complications of anti-PD-1/PD-L1 immune checkpoint antibodies. Curr Opin Oncol. 2016;28:254–263. doi: 10.1097/CCO.0000000000000290. [DOI] [PubMed] [Google Scholar]
- 24.Naidoo J, Schindler K, Querfeld C, et al. Autoimmune bullous skin disorders with immune checkpoint inhibitors targeting PD-1 and PD-L1. Cancer Immunol Res. 2016;4:383–389. doi: 10.1158/2326-6066.CIR-15-0123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Zarbo A, Belum VR, Sibaud V, et al. Immune-related alopecia (areata and universalis) in cancer patients receiving immune checkpoint inhibitors. Br J Dermatol. 2017;176:1649–1652. doi: 10.1111/bjd.15237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Barbosa NS, Wetter DA, Wieland CN, et al. Scleroderma induced by pembrolizumab: A case series. Mayo Clin Proc. 2017;92:1158–1163. doi: 10.1016/j.mayocp.2017.03.016. [DOI] [PubMed] [Google Scholar]
- 27.Sowerby L, Dewan AK, Granter S, et al. Rituximab treatment of nivolumab-induced bullous pemphigoid. JAMA Dermatol. 2017;153:603–605. doi: 10.1001/jamadermatol.2017.0091. [DOI] [PubMed] [Google Scholar]
- 28.Coleman E, Ko C, Dai F, et al. Inflammatory eruptions associated with immune checkpoint inhibitor therapy: A single-institution, retrospective analysis with stratification of reactions by toxicity and implications for management. J Am Acad Dermatol. 2019;80:990–997. doi: 10.1016/j.jaad.2018.10.062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Teulings HE, Limpens J, Jansen SN, et al. Vitiligo-like depigmentation in patients with stage III-IV melanoma receiving immunotherapy and its association with survival: A systematic review and meta-analysis. J Clin Oncol. 2015;33:773–781. doi: 10.1200/JCO.2014.57.4756. [DOI] [PubMed] [Google Scholar]
- 30.Kosche C, Mohindra N, Choi JN. Vitiligo in a patient undergoing nivolumab treatment for non-small cell lung cancer. JAAD Case Rep. 2018;4:1042–1044. doi: 10.1016/j.jdcr.2018.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Liu RC, Consuegra G, Chou S, et al. Vitiligo-like depigmentation in oncology patients treated with immunotherapies for nonmelanoma metastatic cancers. Clin Exp Dermatol. doi: 10.1111/ced.13867. epub ahead of print on January 7, 2019. [DOI] [PubMed] [Google Scholar]
- 32.Lolli C, Medri M, Ricci M, et al. Vitiligo-like lesions in a patient treated with nivolumab for renal cell carcinoma. Medicine (Baltimore) 2018;97:e13810. doi: 10.1097/MD.0000000000013810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Nishino K, Ohe S, Kitamura M, et al. Nivolumab induced vitiligo-like lesions in a patient with metastatic squamous cell carcinoma of the lung. J Thorac Dis. 2018;10:E481–E484. doi: 10.21037/jtd.2018.05.104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Uenami T, Hosono Y, Ishijima M, et al. Vitiligo in a patient with lung adenocarcinoma treated with nivolumab: A case report. Lung Cancer. 2017;109:42–44. doi: 10.1016/j.lungcan.2017.04.019. [DOI] [PubMed] [Google Scholar]
- 35.Yin ES, Totonchy MB, Leventhal JS. Nivolumab-associated vitiligo-like depigmentation in a patient with acute myeloid leukemia: A novel finding. JAAD Case Rep. 2017;3:90–92. doi: 10.1016/j.jdcr.2016.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Zarogoulidis P, Huang H, Tsiouda T, et al. Immunotherapy “shock” with vitiligo due to nivolumab administration as third line therapy in lung adenocarcinoma. Respir Med Case Rep. 2017;22:283–286. doi: 10.1016/j.rmcr.2017.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Zhao ZM, Liu SC, Xu XJ, et al. Treatment of skin reaction induced by nivolumab combined with radiotherapy in non-small cell lung cancer: A case report. Chin Med Sci J. 2018;33:183–187. doi: 10.24920/31805. [DOI] [PubMed] [Google Scholar]
- 38.Rodríguez-Lomba E, Molina-López I, Suárez-Fernández R, et al. Vitiligo-like lesions and immune checkpoint inhibition therapy: Is it truly an adverse event exclusive to patients with melanoma? Clin Exp Dermatol. 2018;43:598–599. doi: 10.1111/ced.13382. [DOI] [PubMed] [Google Scholar]
- 39.Salati M, Baldessari C, Calabrese F, et al. Nivolumab-induced impressive response of refractory pulmonary sarcomatoid carcinoma with brain metastasis. Case Rep Oncol. 2018;11:615–621. doi: 10.1159/000492666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Dumbrava EI, Ivan D, Subbiah V. Hypopigmented skin lesions after immunotherapy. JAMA Oncol. 2018;4:1118–1119. doi: 10.1001/jamaoncol.2018.0186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Khoja L, Day D, Wei-Wu Chen T, et al. Tumour- and class-specific patterns of immune-related adverse events of immune checkpoint inhibitors: A systematic review. Ann Oncol. 2017;28:2377–2385. doi: 10.1093/annonc/mdx286. [DOI] [PubMed] [Google Scholar]
- 42.Boutros C, Tarhini A, Routier E, et al. Safety profiles of anti-CTLA-4 and anti-PD-1 antibodies alone and in combination. Nat Rev Clin Oncol. 2016;13:473–486. doi: 10.1038/nrclinonc.2016.58. [DOI] [PubMed] [Google Scholar]
- 43.Sznol M, Ferrucci PF, Hogg D, et al. Pooled analysis safety profile of nivolumab and ipilimumab combination therapy in patients with advanced melanoma. J Clin Oncol. 2017;35:3815–3822. doi: 10.1200/JCO.2016.72.1167. [DOI] [PubMed] [Google Scholar]
- 44.Weber JS, Hodi FS, Wolchok JD, et al. Safety profile of nivolumab monotherapy: A pooled analysis of patients with advanced melanoma. J Clin Oncol. 2017;35:785–792. doi: 10.1200/JCO.2015.66.1389. [DOI] [PubMed] [Google Scholar]
- 45.Min Lee CK, Li S, Tran DC, et al. Characterization of dermatitis after PD-1/PD-L1 inhibitor therapy and association with multiple oncologic outcomes: A retrospective case-control study. J Am Acad Dermatol. 2018;79:1047–1052. doi: 10.1016/j.jaad.2018.05.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Grangeon M, Tomasini P, Chaleat S, et al. Association between immune-related adverse events and efficacy of immune checkpoint inhibitors in non-small-cell lung cancer. Clin Lung Cancer. doi: 10.1016/j.cllc.2018.10.002. Epub ahead of print on October 11, 2018. [DOI] [PubMed] [Google Scholar]
- 47.Manson G, Norwood J, Marabelle A, et al. Biomarkers associated with checkpoint inhibitors. Ann Oncol. 2016;27:1199–1206. doi: 10.1093/annonc/mdw181. [DOI] [PubMed] [Google Scholar]
- 48.Oh DY, Cham J, Zhang L, et al. Immune toxicities elicited by CTLA-4 blockade in cancer patients are associated with early diversification of the T-cell repertoire. Cancer Res. 2017;77:1322–1330. doi: 10.1158/0008-5472.CAN-16-2324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Cousin S, Italiano A. Molecular pathways: Immune checkpoint antibodies and their toxicities. Clin Cancer Res. 2016;22:4550–4555. doi: 10.1158/1078-0432.CCR-15-2569. [DOI] [PubMed] [Google Scholar]
- 50.Tetzlaff MT, Nagarajan P, Chon S, et al. Lichenoid dermatologic toxicity from immune checkpoint blockade therapy: A detailed examination of the clinicopathologic features. Am J Dermatopathol. 2017;39:121–129. doi: 10.1097/DAD.0000000000000688. [DOI] [PubMed] [Google Scholar]
- 51.Gaitanis G, Bassukas ID. Immunocryosurgery for non-superficial basal cell carcinoma: A prospective, open-label phase III study for tumours ≤ 2 cm in diameter. Acta Derm Venereol. 2014;94:38–44. doi: 10.2340/00015555-1609. [DOI] [PubMed] [Google Scholar]
- 52.Goldinger SM, Stieger P, Meier B, et al. Cytotoxic cutaneous adverse drug reactions during anti-PD-1 therapy. Clin Cancer Res. 2016;22:4023–4029. doi: 10.1158/1078-0432.CCR-15-2872. [DOI] [PubMed] [Google Scholar]
- 53.Friedman CF, Proverbs-Singh TA, Postow MA. Treatment of the immune-related adverse effects of immune checkpoint inhibitors: A review. JAMA Oncol. 2016;2:1346–1353. doi: 10.1001/jamaoncol.2016.1051. [DOI] [PubMed] [Google Scholar]
- 54.Curry JL, Tetzlaff MT, Nagarajan P, et al. Diverse types of dermatologic toxicities from immune checkpoint blockade therapy. J Cutan Pathol. 2017;44:158–176. doi: 10.1111/cup.12858. [DOI] [PubMed] [Google Scholar]
- 55.Hasan Ali O, Diem S, Markert E, et al. Characterization of nivolumab-associated skin reactions in patients with metastatic non-small cell lung cancer. OncoImmunology. 2016;5:e1231292. doi: 10.1080/2162402X.2016.1231292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Shi VJ, Rodic N, Gettinger S, et al. Clinical and histologic features of lichenoid mucocutaneous eruptions due to anti-programmed cell death 1 and anti-programmed cell death ligand 1 immunotherapy. JAMA Dermatol. 2016;152:1128–1136. doi: 10.1001/jamadermatol.2016.2226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Kaunitz GJ, Loss M, Rizvi H, et al. Cutaneous eruptions in patients receiving immune checkpoint blockade: Clinicopathologic analysis of the nonlichenoid histologic pattern. Am J Surg Pathol. 2017;41:1381–1389. doi: 10.1097/PAS.0000000000000900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Siegel J, Totonchy M, Damsky W, et al. Bullous disorders associated with anti-PD-1 and anti-PD-L1 therapy: A retrospective analysis evaluating the clinical and histopathologic features, frequency, and impact on cancer therapy. J Am Acad Dermatol. 2018;79:1081–1088. doi: 10.1016/j.jaad.2018.07.008. [DOI] [PubMed] [Google Scholar]
- 59.Lim SY, Lee JH, Gide TN, et al. Circulating cytokines predict immune-related toxicity in melanoma patients receiving anti-PD-1-based immunotherapy. Clin Cancer Res. 2019;25:1557–1563. doi: 10.1158/1078-0432.CCR-18-2795. [DOI] [PubMed] [Google Scholar]
- 60.Naqash AR, Yang LV, Sanderlin EJ, et al. Interleukin-6 as one of the potential mediators of immune-related adverse events in non-small cell lung cancer patients treated with immune checkpoint blockade: Evidence from a case report. Acta Oncol. 2018;57:705–708. doi: 10.1080/0284186X.2017.1406668. [DOI] [PubMed] [Google Scholar]
- 61.Kim ST, Tayar J, Trinh VA, et al. Successful treatment of arthritis induced by checkpoint inhibitors with tocilizumab: A case series. Ann Rheum Dis. 2017;76:2061–2064. doi: 10.1136/annrheumdis-2017-211560. [DOI] [PubMed] [Google Scholar]
- 62.Uemura M, Trinh VA, Haymaker C, et al. Selective inhibition of autoimmune exacerbation while preserving the anti-tumor clinical benefit using IL-6 blockade in a patient with advanced melanoma and Crohn’s disease: A case report. J Hematol Oncol. 2016;9:81. doi: 10.1186/s13045-016-0309-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Brudno JN, Kochenderfer JN. Toxicities of chimeric antigen receptor T cells: Recognition and management. Blood. 2016;127:3321–3330. doi: 10.1182/blood-2016-04-703751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Chen F, Teachey DT, Pequignot E, et al. Measuring IL-6 and sIL-6R in serum from patients treated with tocilizumab and/or siltuximab following CAR T cell therapy. J Immunol Methods. 2016;434:1–8. doi: 10.1016/j.jim.2016.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Maude SL, Barrett D, Teachey DT, et al. Managing cytokine release syndrome associated with novel T cell-engaging therapies. Cancer J. 2014;20:119–122. doi: 10.1097/PPO.0000000000000035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Rotz SJ, Leino D, Szabo S, et al. Severe cytokine release syndrome in a patient receiving PD-1-directed therapy. Pediatr Blood Cancer. 2017;64:e26642. doi: 10.1002/pbc.26642. [DOI] [PubMed] [Google Scholar]
- 67.Maurer M, Rosén K, Hsieh HJ, et al. Omalizumab for the treatment of chronic idiopathic or spontaneous urticaria. N Engl J Med. 2013;368:924–935. doi: 10.1056/NEJMoa1215372. [DOI] [PubMed] [Google Scholar]
- 68.Phillips GS, Freites-Martinez A, Wu J, et al. Clinical characterization of immunotherapy-related pruritus in 79 cancer patients in an oncodermatology clinic. JAMA Dermatol. 2019;155:249–251. doi: 10.1001/jamadermatol.2018.4560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Foroutan N, Etminan A, Nikvarz N, et al. Comparison of pregabalin with doxepin in the management of uremic pruritus: A randomized single blind clinical trial. Hemodial Int. 2017;21:63–71. doi: 10.1111/hdi.12455. [DOI] [PubMed] [Google Scholar]
- 70.Santini D, Vincenzi B, Guida FM, et al. Aprepitant for management of severe pruritus related to biological cancer treatments: A pilot study. Lancet Oncol. 2012;13:1020–1024. doi: 10.1016/S1470-2045(12)70373-X. [DOI] [PubMed] [Google Scholar]
- 71.Santini FC, Rizvi H, Plodkowski AJ, et al. Safety and efficacy of re-treating with immunotherapy after immune-related adverse events in patients with NSCLC. Cancer Immunol Res. 2018;6:1093–1099. doi: 10.1158/2326-6066.CIR-17-0755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Faje AT, Lawrence D, Flaherty K, et al. High-dose glucocorticoids for the treatment of ipilimumab-induced hypophysitis is associated with reduced survival in patients with melanoma. Cancer. 2018;124:3706–3714. doi: 10.1002/cncr.31629. [DOI] [PubMed] [Google Scholar]
- 73.Arbour KC, Mezquita L, Long N, et al. Impact of baseline steroids on efficacy of programmed cell death-1 and programmed death-ligand 1 blockade in patients with non-small-cell lung cancer. J Clin Oncol. 2018;36:2872–2878. doi: 10.1200/JCO.2018.79.0006. [DOI] [PubMed] [Google Scholar]
- 74.Kumar V, Chaudhary N, Garg M, et al. Current diagnosis and management of immune related adverse events (irAEs) induced by immune checkpoint inhibitor therapy. Front Pharmacol. 2017;8:49. doi: 10.3389/fphar.2017.00049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Collins LK, Chapman MS, Carter JB, et al. Cutaneous adverse effects of the immune checkpoint inhibitors. Curr Probl Cancer. 2017;41:125–128. doi: 10.1016/j.currproblcancer.2016.12.001. [DOI] [PubMed] [Google Scholar]
- 76.Sibaud V, Lebœuf NR, Roche H, et al. Dermatological adverse events with taxane chemotherapy. Eur J Dermatol. 2016;26:427–443. doi: 10.1684/ejd.2016.2833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Villadolid J, Amin A. Immune checkpoint inhibitors in clinical practice: Update on management of immune-related toxicities. Transl Lung Cancer Res. 2015;4:560–575. doi: 10.3978/j.issn.2218-6751.2015.06.06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Champiat S, Lambotte O, Barreau E, et al. Management of immune checkpoint blockade dysimmune toxicities: A collaborative position paper. Ann Oncol. 2016;27:559–574. doi: 10.1093/annonc/mdv623. [DOI] [PubMed] [Google Scholar]
- 79.Spain L, Diem S, Larkin J. Management of toxicities of immune checkpoint inhibitors. Cancer Treat Rev. 2016;44:51–60. doi: 10.1016/j.ctrv.2016.02.001. [DOI] [PubMed] [Google Scholar]
- 80.Oetjen LK, Mack MR, Feng J, et al. Sensory neurons co-opt classical immune signaling pathways to mediate chronic itch. Cell. 2017;171:217.e13–228.e13. doi: 10.1016/j.cell.2017.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]